
Purpose
High-dose-rate (HDR) brachytherapy (BT) offers precise dose delivery with minimal exposure to surrounding healthy tissue, establishing it as a standard of care for diverse carcinomas [1, 2]. Compared with external beam radiation therapy (EBRT), HDR-BT is particularly effective for superficial lesions in anatomically complex areas, such as skin lesions with high surface curvature, due to its close-range dose delivery and customizable catheter placement for improved dose conformality.
Conventional HDR-BT approaches for skin lesions include surface flaps, such as the Freiburg Flap (FF) applicator [1, 3] (Elekta Instrument AB, Stockholm, Sweden) and custom-made surface mold [4]. The FF applicator is a flexible mesh embedded with spherical silicone beads, creating channels spaced 10 mm apart through which catheters are threaded to guide HDR source during treatment. Immobilization is achieved by securing the applicator to a thermo-plastic mask customized during CT simulation, a standard device also used in EBRT. The surface mold uses a similar immobilization method, but allows variable channel spacing for enhanced dose conformality. Both approaches have demonstrated efficacy for superficial tumors located within 5 mm of the skin surface, including non-melanoma skin cancer [5], mycosis fungoides [6], and selected shallow lesions of the chest wall [7], head and neck [8, 9], and extremities [10, 11].
Traditional applicators still exhibit limitations. In this study, a 72-year-old patient was diagnosed with T1N0 cutaneous neuroendocrine carcinoma (Merkel cell) and referred for radiation therapy. The treatment area included both dorsal and palmar sides of the right hand as well as inter-digital spaces. The complex anatomy precluded EBRT, leaving HDR-BT as the sole viable option. Though FF beads were too large to adequately cover the areas between the fingers [12] and despite efforts to mold the thermo-plastic mask closely to the skin, substantial air gaps remained, resulting in compromised dose distribution.
Recent developments in 3D printing have shown advantages in EBRT, improving both dosimetry [8, 13, 14] and patient setup reproducibility [15]; 3D-printed parts are generated from patient’s CT scans and their patient-specific design increases the likelihood of minimizing air gaps. The rigid or semi-rigid material may also improve immobilization consistency. Together, these features align with the requirements of patient-specific HDR-BT, particularly for lesions located in highly curved, narrow anatomical areas, limitations that traditional skin applicators fail to address.
Leveraging these capabilities, we developed a novel 3D-printed skin applicator for HDR-BT to treat Merkel cell carcinoma. We demonstrated its dosimetric and immobilization advantages, and established a streamlined workflow that optimized clinical staff resources from simulation to treatment.
Material and methods
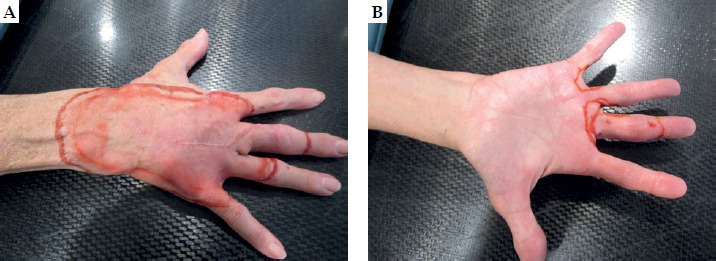
A 72-year-old female patient with T1N0 cutaneous neuroendocrine carcinoma (Merkel cell) was referred for HDR-BT. At consultation, a radiation oncologist outlined all visible lesions on the right hand, including the dorsal and palmar surfaces, inter-digital spaces, and portions of the index, middle, and ring fingers (Figure 1). Treatment areas were then marked with a 10 mm expansion margin from the lesion boundaries. Prior to CT simulation, a radio-opaque wire was placed along these skin markings to guide delineation of planning target volume (PTV). The patient was positioned head-first prone, with the right arm extended overhead to avoid imaging the torso. A high-resolution CT scan (1.25 mm slice thickness) was acquired to enable precise catheter digitization, and images were imported into the Eclipse treatment planning system (TPS) (Varian, Palo Alto, CA). The hand surface was contoured using appropriate window and level settings. Subsequently, PTV was created by extending the hand surface contour 4 mm subcutaneously over wire-marked regions. A single fraction of 8 Gy was prescribed [16, 17], with at least 90% of PTV (D90%) receiving a prescription dose and maximum dose to the most irradiated 0.03 cc (D0.03cc) of PTV kept below 140% of the prescription dose.
The applicator structure was initially generated in the Eclipse TPS by expanding the hand surface contour 10 mm outward. It was then exported to 3D Brachy software (Adaptiiv Medical Technologies, Halifax, Canada) for refinement and catheter channel design. To facilitate accurate modeling, the applicator was divided along the coronal plane into palmer and dorsal components (Figure 2A). Catheter channels were designed for Best Medical ProGuide (Best Medical International, Springfield, VA) catheters (outer diameter of 1.6 mm), using a 2 mm channel diameter to ensure adequate clearance and secure placement. Channels were then embedded within the applicator, positioned 5 mm from the skin surface, with an inter-channel spacing of 10 mm. Numbers and positions of the catheters were optimized to prioritize target coverage, with selective inter-channel spacing adjustment made to mitigate dose hot spots in the treatment plan. Catheter trajectories complied with the software’s curvature limits to reduce the risk of source obstruction during treatment delivery.
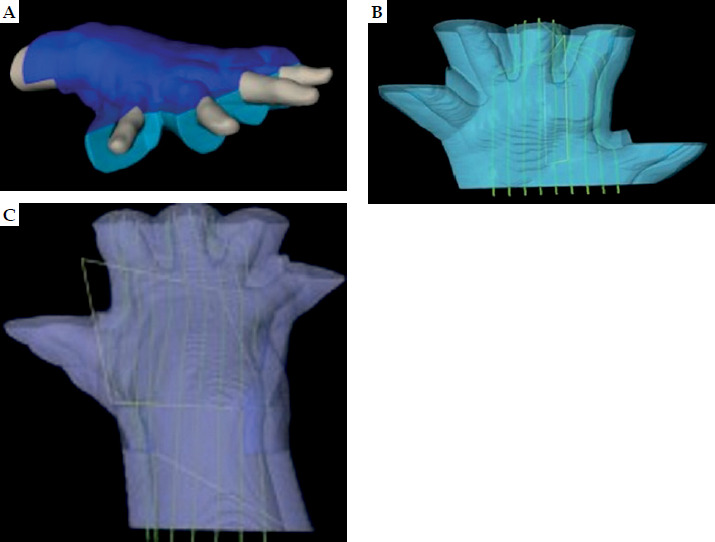
Fig. 2
Skin applicator design in 3D Brachy software. A) Palmar (cyan) and dorsal (blue) components, B) palmar component with catheter channels, and C) dorsal component with catheter channels
Following completion of the design, the applicator was exported to Adaptiiv On Demand (AOD), a third-party printing service by Adaptiiv Medical Technologies Inc. An FDA-approved, bio-compatible clear resin (1.16 g/cm3) was selected for applicator fabrication using a stereolithography 3D printer (Formlabs, Somerville, MA). Quality assurance (QA) was performed to verify print dimensions and exclude defects, such as air bubbles within the applicator. Subsequently, the patient underwent a second CT simulation with the applicator and catheters in place, as shown in Figure 3, using the same setup position and imaging parameters as the initial simulation. Images were imported into the Oncentra Brachy TPS (Elekta AB, Stockholm, Sweden), where catheters were digitized to reproduce the design in 3D Brachy. Source dwell positions were activated and optimized at 2 mm intervals to meet planning objectives. Dose distribution was calculated according to the American Association of Physicists in Medicine (AAPM) Task Group (TG) 43 formalism [18]. Prior to treatment, a dry run was performed to verify source travel, and catheter lengths were confirmed using a source position simulator (SPS). Treatment was subsequently delivered using a Flexitron HDR-BT afterloader (Elekta AB, Stockholm, Sweden).

Results
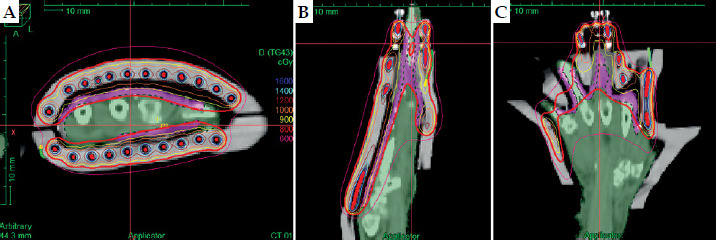
The 3D-printed skin applicator incorporated 27 catheter channels, with translucent resin providing clear visualization of the catheter placement (Figure 3). The print surface was smooth, and the QA results confirmed a defect-free print with no air bubbles within the applicator. Air gaps between the applicator and skin surface were less than 5 mm for both palmer and dorsal components. The planning results achieved PTV coverage of 98.6% at D90% and 96.7% at D95%, with D0.03cc of 135.6%. Figure 4 illustrates the dose distribution. The dry run verified unobstructed source travel, and differences between expected and measured SPS values were within ± 1 mm, meeting the AAPM TG-56 and TG-59 specifications [19, 20]. The treatment was delivered successfully using a 5 Ci Iridium-192 (192Ir) HDR source, with a total treatment time of 51 minutes (15 minutes for patient’s setup and 36 minutes for delivery). The patient maintained a stable position throughout the treatment. At 1-year follow-up, clinical evaluation and imaging showed no evidence of disease recurrence or radiation-induced toxicity.
Discussion
In this study, we presented a patient-specific 3D-printed applicator as a novel solution for treating complex skin lesions in HDR-BT. It enabled dose delivery to inter-digital areas, which were inaccessible to traditional FF or surface mold techniques. Derived from the patient’s CT scan, the applicator minimized air gaps and improved dose conformality. The semi-rigid, translucent resin facilitated reproducible setup and allowed visualization of catheter positions relative to the target, enhancing the accuracy and safety of treatment delivery. Additionally, the workflow optimized physicist resources by eliminating manual, labor-intensive applicator fabrication, while adhering to standard simulation-to-treatment timelines. Ultimately, this study offers a feasible pathway for clinics without in-house printing capabilities to deliver accurate and effective care for patients with challenging superficial lesions.
Air gaps between the skin and applicator are a known challenge that compromises plan quality [5, 21]. To mitigate this obstacle, we implemented an iterative, trial-and-error approach to determine optimal CT window and level settings. A range of –700 to +300 Hounsfield units (HU) was adopted to generate consistent hand contour across most regions, which was used for applicator structure expansion. However, small air gaps persisted at the middle fingertip. To improve conformity in that area, an additional 1.1 mm layer of dental wax was manually applied. Unlike the conventional FF applicator that requires a thermo-plastic mask for immobilization, introducing both mask-to-skin and applicator-to-mask air gaps, the 3D-printed applicator was placed directly on the patient’s skin, eliminating additional sources of errors and simplifying the setup process.
The applicator was separated as dorsal and palmer halves to further enhance planning and treatment efficacy. An enclosed “glove” applicator design was initially attempted, but cavities near the palm and fingers were modelled as extreme curvatures by the 3D Brachy software, resulting in catheter placement inaccuracies. The narrowing near the fingertips also impeded hand insertion. In contrast, the open geometry of the split design facilitated hand placement and enabled visual confirmation of catheter alignment with the treatment plan, improving setup accuracy. Additionally, fabrication efficiency was enhanced by printing both halves simultaneously.
Clear resin was selected for its combined dosimetric and clinical advantages. First, it is an FDA-approved, bio-compatible material, safe for direct patient contact. With a density of 1.16 g/cm3, it is tissue-equivalent and complies with the AAPM TG-43 dose calculation formalism [18]. Second, its semi-rigid property provides superior hand immobilization compared with soft FF applicator, thereby reducing inter-fractional variability in air gap locations, a demonstrated benefit of 3D-printed devices in EBRT [15]. The enhanced setup reproducibility is particularly valuable for complex treatment setups, such as ours, further supporting effective treatment delivery. Third, the material’s translucency allows visualization of catheter placement, offering direct confirmation of catheters adequately covering the skin-marked lesions and aligning with the planned depths, thereby ensuring setup accuracy during treatment delivery.
This work highlights future directions for advancing 3D-printing applications in HDR brachytherapy. As the most complex superficial lesion treated at our center to date and our first attempt using a novel 3D-printing workflow, a 1 mm clearance was added at the fingertip to ensure proper fit. This margin can be safely removed in future cases, eliminating the need for manual dental wax application. Treatment efficiency can also be improved by using a 10 Ci 192Ir source. In this study, a 5 Ci was employed, as the scheduled source exchange would not have met treatment start timelines. The workflow established here has already been extended to additional patients, paving the way for evaluation of treatment efficacy among a larger cohort in future studies. Although our patient did well at one-year follow-up, she remains at potential high-risk for both local and distant recurrence, and therefore requires close surveillance.
Conclusions
We presented a novel approach for treating complex Merkel cell carcinoma of the hand, which could not be effectively treated with conventional techniques. The patient-specific, 3D-printed skin applicator reduced air gaps, improved dose conformity, and significantly enhanced setup reproducibility through its semi-rigid, translucent resin. The treatment was delivered within the standard simulation-to-treatment timeline, while clinical staff resources were substantially optimized by eliminating the manual fabrication process of traditional skin applicators. At follow-up, the patient showed no cancer recurrence or toxicity. The workflow offers a feasible option for clinics without in-house 3D-printing capabilities to deliver accurate, effective care for challenging superficial lesions in high-dose-rate brachytherapy.








