Coronary calcifications constitute a significant challenge for percutaneous coronary interventions (PCI) – particularly in the elderly – and proper selection of calcium-modifying techniques is of paramount importance [1, 2]. For crossable lesions, two lithotripsy(IVL)-based modalities are currently available: Shockwave IVL (Shockwave Medical Inc., US) and non-energy-based IVL LithIX (Elixir Medical, US) [3]. The latter is based on Hertz-contact (HC) stress phenomenon and does not require an external energy source. It is designed to have better deliverability compared to Shockwave. Despite LithIX longer length (14 mm vs. 12 mm of Shockwave) and larger crossing profile (it depends on LithIX balloon diameter: ranging from 1.17 mm for 1.5 mm up to 1.45 mm for 3.5 mm, contrary to 1.1 mm for all sizes of Shockwave balloons), it is mounted on a semi-compliant balloon, without energy emitters housed inside (Supplementary file) [4].
Herein, we present a 90-year-old male patient with non-ST elevation myocardial infarction in the course of multivessel coronary artery disease. Initially, the patient was admitted due to an intermediate-low risk pulmonary embolism in the postoperative period, related to femoral cervix fracture. The following day, he experienced chest pain with dynamic ECG changes in precordial leads, heart failure (EF19%) and a marked troponin T rise (42–> 1993 U/l). An urgent coronary angiography revealed severely calcified stenoses in the proximal left anterior descending artery (LAD) (TIMI 2 flow) and the right coronary artery (RCA). The decision was made to proceed with an immediate, intravascular ultrasound-guided PCI of the LAD and, due to the patient’s orthopnoe, staged PCI of the RCA. Following 2.5/15.0 mm non-compliant (NC) balloon predilatation and delivery of 80 IVL pulses (Shockwave 3.5/12.0 mm), a sirolimus-eluting stent was implanted (Orsiro Mission 3.0/40 mm) in the LAD and postdilated with an NC 4.0/15.0 mm balloon (Figures 1 A, B). Two days later, following clinical stabilization, an optical coherence tomography (OCT)-guided PCI of the RCA was performed (7F right transradial approach) (Figures 1 C, D). After lesion predilatation with a 2.5 NC balloon, an OCT was performed (calcium score-4 points). Given the lesion length and anticipated deliverability challenges, a HC-IVL LithIX was used for plaque modification instead of Shockwave IVL. Despite further predilatations with a 3.5/15.0 mm NC balloon, HC-IVL could not be advanced through the bend in the 2nd segment of the RCA. Unfortunately, there was no 7F guide extension catheter on the shelf, a buddy-wire technique also failed after using once-expanded LithIX balloon. As a result, only the proximal part of the lesion was modified with a 3.5/14 mm HC-IVL (gradual inflations 0–5 atm, followed by 14 atm for 30 s), while the distal part was modified using a 3.5/15.0 mm NC balloon (24 atm). A postprocedural OCT revealed minor calcium cracks (within a 270-degree calcium arch in the proximal RCA) and a subintimal dissection (2nd segment of the RCA). Subsequently, two overlapping zotarolimus-eluting stents (Onyx Trustar 4.0/18 and 4.0/26 mm) were implanted and postdilated with a 4.0/15.0 mm NC balloon. In a final OCT, stents expansion exceeded 90%. The further hospital stay was uneventful, the patient was discharged after 10 days. The present case demonstrates that staged, imaging-guided and patient-tailored approach to calcified lesions with balloon-based calcium-modifying techniques may be safe and effective in multimorbid elderly patients. HC-IVL LithIX may complement existing balloon-based calcium-modifying devices, particularly for extended tight lesions (potentially resistant to pulses delivered by a single Shockwave balloon, provided it could cross the lesion). It is worth noting that larger HC-IVL balloon deliverability may be also challenging due to their crossing profile.
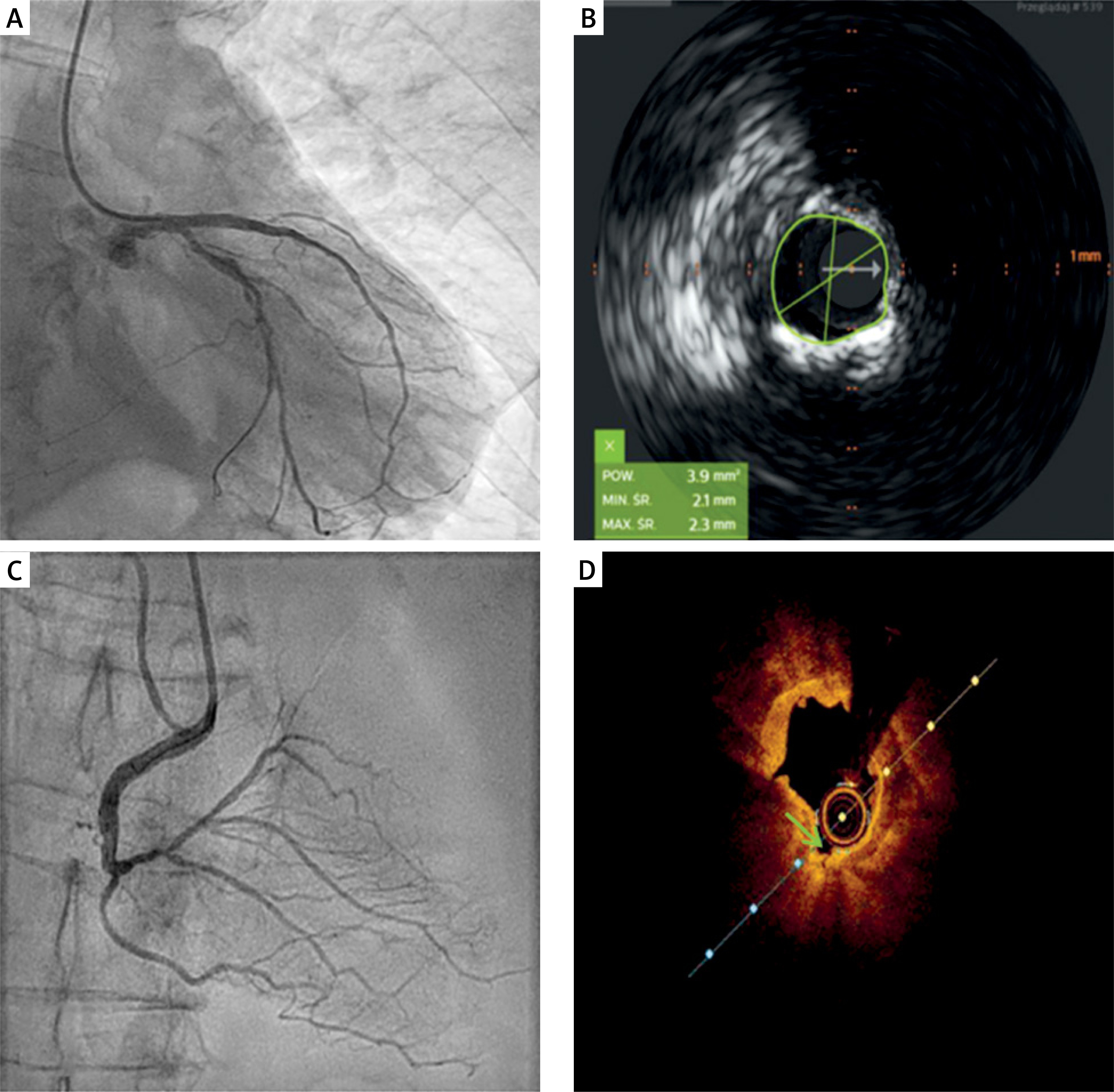
Figure 1
A – Final angiographic result following intravascular ultrasound-guided and Shockwave-assisted PCI of the left anterior descending artery. B – Intravascular ultrasound image, 270-degree calcium arch in the left anterior descending artery. C – Final angiographic result following optical coherence tomography-guided and LithIX-assisted PCI of the right coronary artery. D – Optical coherence tomography showing only minor tissue cracks in the right coronary artery following Hertz-contact non-energy IVL LithIX inflations (green arrow)