
Introduction
Pancreatic cancer (PC) is regarded as one of the most deadliest malignancies, demonstrating an overall survival (OS) rate of no more than 13% across a five-year span. As reported by GLOBOCAN 2024, it represents the third leading cause of cancer-related deaths [1]. Low survival rates are primarily linked to diagnoses at advanced stages, with approximately 20% of patients receiving a diagnosis of resectable disease. Among the factors contributing to the development of PC, the authors identify age, cigarette smoking, obesity, excessive alcohol consumption, diabetes mellitus, pancreatitis, and a family history of PC [2, 3]. In the majority of cases, early PC remains asymptomatic. Potential symptoms may include abdominal pain and distension, weight loss, dyspepsia, dysphagia, constipation, nausea, vomiting, jaundice, and new-onset diabetes. Nevertheless, these symptoms typically present during the advanced stages of the disease [4, 5]. Currently, there is no standardized screening protocol for PC. Some guidelines recommend the use of endoscopic ultrasonography or magnetic resonance imaging for individuals who have multiple close relatives diagnosed with PC, those who carry a pathogenic variant in one of the high-risk PC susceptibility genes, or individuals with a personal history of pancreatic cysts [2]. Histopathologically, approximately 90% of PC are classified as pancreatic ductal adenocarcinomas (PDAC). The neoplastic precursor lesions that lead to PDAC include pancreatic intraepithelial neoplasia (PanIN), intraductal papillary mucinous neoplasms, and mucinous cystic neoplasms. Molecular studies indicate that the majority of PDAC originate from PanIN, a condition that current imaging modalities are unable to detect [6]. Carbohydrate 19-9 antigen (CA19-9) is frequently expressed in the cells of the pancreaticobiliary system. In patients diagnosed with cancer, the serum concentration of CA19-9 is commonly elevated, exhibiting its highest sensitivity and specificity in individuals with PC; however, it may also be elevated in various other medical conditions [7]. Another widely used, yet non-specific, marker in diagnosing and assessing PC is carcinoembryonic antigen (CEA) [8].
One hallmark of carcinogenesis is tumour-promoting inflammation [9]. In recent decades, the role of inflammation in the development, progression, and response to chemotherapy of cancer has experienced a renewed surge of interest [10]. In PC, immunotherapy is limited to about 1% of patients with microsatellite instability-high or mismatch repair deficient tumours. In other cases, it fails to achieve effectiveness, likely due to a highly immunosuppressive and dense tumour microenvironment [11]. Nonetheless, various aspects of inflammation and the immune response in PC patients are of great interest. Some studies focus on pre-treatment inflammatory markers and their prognostic significance [12].
This study aimed to analyse the inflammatory status of patients with PC before the initial course of chemotherapy and to identify the most accurate systemic inflammation index for predicting OS.
Material and methods
Patient selection and evaluation
A single-centre retrospective analysis encompassing 550 medical records from patients diagnosed with PC (C25, as classified by the International Statistical Classification of Diseases and Related Health Problems) was conducted. The patients received treatment at the National Medical Institute of the Ministry of the Interior and Administration in Warsaw from 2012 to 2024. From the total of 550 medical records, 310 were selected as eligible for inclusion in the study [13]. As this was a retrospective study, no prior protocol was established to determine the study size. The number of included patients was based on the total number of eligible medical records available during the study period, after applying the predefined inclusion and exclusion criteria. Inclusion criteria included: age ≥ 18 years [14], histological or cytological confirmation of PC [15], receiving two or more full cycles of chemotherapy [16], and no clinical evidence of infection at chemotherapy qualification [16, 17]. The exclusion criteria included:
The patients were categorized into two cohorts: those treated with palliative intent from the start (palliative group, n = 150) and those treated with curative intent (adjuvant group, n = 160).
The data under analysis encompassed various parameters, including but not limited to gender, age, height, weight, body mass index (BMI), body surface area [20], performance status (PS) [21], medical history (including other diseases, cigarette smoking, prior primary tumours, and family history of malignancies). Furthermore, the examined pathological variables were tumour site, tumour size, nodal involvement, tumour stage, resection margin, angioinvasion, and neuroinvasion [15]. Treatment variables accounted for types of surgical procedures, vascular reconstruction, as well as adjuvant and palliative chemotherapy [16], along with associated side effects. Additionally, laboratory findings preceding the initial course of chemotherapy, calculated parameters prior to the first chemotherapy course, disease-free survival (DFS), progression-free survival (PFS), and OS.
Tumour staging was evaluated in accordance with the criteria outlined in the American Joint Cancer Committee Staging Manual, 8th edition [22]. Progression and recurrence of the disease were identified utilizing the computed tomography protocol for the chest, abdomen, and pelvis [16]. The primary endpoint of the study was OS, which was calculated from the date of histologically confirmed diagnosis obtained through biopsies or surgical procedures to the date of last follow-up or the occurrence of death. The date of death was ascertained by reviewing the patients’ medical records.
Inflammatory status parameters
Blood samples were collected from patients during chemotherapy qualification, either on the first day of chemotherapy or the day before. At that time, patients did not exhibit any symptoms of inflammation (i.e., upper respiratory tract inflammation, pneumonia, gastroenteritis). The parameters of the inflammatory status that were analysed were calculated as follows [23–25]:
Statistical analysis
Results were regarded as significant with a p-value of ≤ 0.05. All statistical analyses were performed using IBM SPSS Statistics 27. Baseline laboratory characteristics and inflammatory indices were summarized for the cohort (n = 310). Due to non-normal distributions, continuous variables were expressed as medians with interquartile ranges (IQR). Categorical variables were reported as frequencies and percentages. Sample sizes varied across parameters due to missing data or assay availability.
Optimal cut-off values for continuous parameters predicting mortality were identified using the maximally selected rank statistic method. This approach evaluated all possible cut points across each parameter’s range, selecting the value that maximized the log-rank statistic to achieve the greatest separation in survival curves between groups. The log-rank test assessed the statistical significance of survival differences.
To evaluate the prognostic significance of each parameter, Cox proportional hazards models were fitted after dichotomizing variables at their optimal cut-offs. Survival time (in months) and event status (death) served as outcomes, with the dichotomized parameter acting as the predictor. Hazard ratios (HR) with 95% CI and p-values were calculated to quantify the strength and significance of the association with mortality. The proportional hazards assumption was tested using Schoenfeld residuals.
The discriminatory ability of dichotomized parameters was assessed through time-dependent receiver operating characteristic curves, with the area under the curve (AUC) calculated at 16 months, which was the median follow-up time. To account for censoring, inverse probability of censoring weighting estimation of the cumulative/dynamic AUC was applied, utilizing marginal weighting to adjust for censoring probability over time. Area under the curve values range from 0.5 (no discrimination) to 1.0 (perfect discrimination), with higher values indicating better predictive accuracy.
Differences in baseline characteristics between patient groups stratified by cut-offs were analysed using appropriate statistical tests, depending on the type and distribution of the variable. For categorical variables, Pearson’s χ2 test and Fisher’s exact test were applied. Continuous variables were compared using the Wilcoxon rank-sum test, as they showed non-normal distributions.
Results
Baseline and clinical characteristics of patients
The studied cohort comprised 310 patients diagnosed with PC, with a modest female predominance of 52.9%. The median age of participants was 65 years, ranging 8–85 years. In the majority of cases, the Eastern Cooperative Oncology Group Performance Status was evaluated during the qualification process for chemotherapy, classified as I (78.5%), which indicates restricted physical activity while still being able to perform light work. A considerable prevalence of comorbidities was noted, including diabetes mellitus (36.6%) and hypertension (51.1%). Furthermore, 31.7% of patients reported a family history of cancer. Notably, 38.4% of patients were diagnosed at stage IV of the disease, with the liver identified as the most common site for metastases (64.7%). Among the remaining patients, 42.3% underwent the Whipple procedure.
For the entire studied cohort, the median OS was determined to be 16.00 months (IQR 10.00–27.00). A pronounced decline in the survival curve was observed during the initial 12–18 months. The median DFS was calculated to be 13.00 months (IQR 8.00–22.00), while the median PFS was noted as 7.00 months (IQR 4.00–11.00).
Determination of cut-off values and the prognostic value of systemic immune-inflammation index, systemic inflammation response index, and inflammatory benchmark index for predicting overall survival
The systemic immune-inflammation index (SII) (cut-off 1657.4) exhibited an AUC of 0.57 and a HR of 1.94 (95% CI: 1.36–2.77, p < 0.001), which indicates a modest discriminatory power and a nearly twofold increase in the risk of mortality beyond the specified threshold. Systemic inflammation response index (SIRI) (cut-off 4.40) demonstrated an AUC equivalent to that of SII (0.57) but presented a higher HR of 2.72 (95% CI: 1.82–4.92, p < 0.001), thereby illustrating a stronger correlation with mortality in spite of the similar levels of discrimination. Systemic immune-inflammation index incorporates the platelet-to-lymphocyte ratio (PLR) alongside the neutrophil-to-lymphocyte ratio (NLR). Accordingly, cut-off values for these parameters were also determined. The neutrophil-to-lymphocyte ratio and PLR attained comparable AUCs of 0.57 and 0.58, respectively; however, both exhibited lower HR of 2.22 and 1.77, respectively (Table 1).
Table 1
Optimal cut-off values and Cox regression results for baseline parameters predicting mortality in patients with pancreatic cancer
| Parameters | n | Optimal cut-off | AUC | Results of Cox regression | ||
|---|---|---|---|---|---|---|
| Estimated vs. reference level | HR (95% CI) | p-value | ||||
| SII [24] | 283 | 1657.40 | 0.57 | > 1657.4 vs. ≤ 1657.4 | 1.94 (1.36, 2.77) | < 0.001 |
| SIRI [23] | 283 | 4.40 | 0.57 | > 4.40 vs. ≤ 4.40 | 2.72 (1.82, 4.92) | < 0.001 |
| IBI [25] | 208 | 10.75 | 0.60 | > 10.75 vs. ≤ 10.75 | 0.35 (0.24, 0.52) | < 0.001 |
| PLR [26] | 307 | 223.23 | 0.58 | > 223.23 vs. ≤ 223.23 | 1.77 (1.32, 2.37) | < 0.001 |
| NLR [27] | 290 | 5.36 | 0.57 | > 5.35 vs. ≤ 5.36 | 2.22 (1.53, 3.22) | < 0.001 |
A high SII significantly predicted a shorter median OS (10 months vs. 16.5 months, p < 0.001). This association was further corroborated in the adjuvant and palliative groups, showing higher statistical significance in the palliative group (p < 0.05 and p < 0.013, respectively). An SII above the cut-off value did not achieve statistical significance in predicting either shorter median PFS (p < 0.285) or shorter DFS (p < 0.07) (Figure 1, 2).
Figure 1
Kaplan-Meier survival curves of overall survival stratified by systemic inflammation response index (A), systemic immune-inflammation
index (B), and inflammatory benchmark index (C) – whole cohort IBI – inflammatory benchmark index, SII – systemic immune-inflammation index, SIRI – systemic inflammation response index
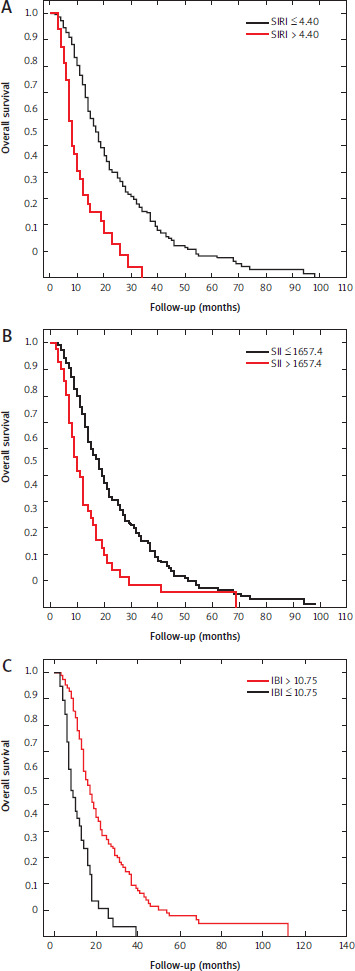
Figure 2
Kaplan-Meier survival curves of overall survival stratified by systemic inflammation response index (A), systemic immune-inflammation
index (B), and inflammatory benchmark index (C) – palliative cohort IBI – inflammatory benchmark index, SII – systemic immune-inflammation index, SIRI – systemic inflammation response index
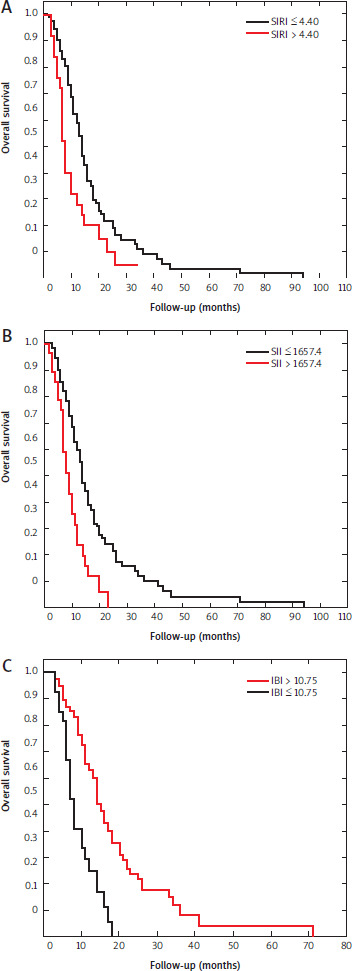
A high SIRI predicted a shorter median OS (8.5 months vs. 16 months, p < 0.001). Nevertheless, this ability was confirmed only in the palliative group with p < 0.006. Systemic inflammation response index above the cut-off value predicted a shorter median PFS (p < 0.03), while it failed to predict shorter DFS (p < 0.265).
Inflammatory benchmark index (IBI) (cut-off 10.75) achieved a slightly better AUC (0.60) and a unique HR of 0.35 (95% CI: 0.24–0.52, p < 0.001), indicating a protective effect above the cut-off, with a 65% reduction in mortality risk (Table 2). A high IBI was a significant predictor of longer median OS (17 months vs. 10 months, p < 0.001), median PFS (9 months vs. 5 months, p < 0.009), and median DFS (14 months vs. 11 months, p < 0.04). Similar to SII, it was a strong predictor of OS in both the adjuvant and palliative groups, with higher statistical significance in the palliative group (p < 0.05 and p < 0.001, respectively).
Table 2
Univariate and multivariate Cox proportional hazards regression analyses of predictors for overall survival in patients with pancreatic cancer
In the univariate analysis, SIRI, SII, and IBI showed a significant association with OS. They were all included in the multivariate analysis, where only IBI remained significantly associated with OS (Table 2).
Baseline and clinical characteristics of patients stratified by systemic immune-inflammation index cut-off
Patients with SII greater than 1657.4 exhibited a higher prevalence of BMI exceeding 23.51 kg/m2 (67.5% vs. 46.0%, p = 0.012), family history of cancer (48.7% vs. 30.1%, p = 0.022), and unresectable tumours (70.7% vs. 47.7%, p = 0.006) compared to those with SII less than or equal to 1657.4. Inflammatory markers were significantly elevated, including white blood cell (WBC) (53.7% vs. 11.2%, p < 0.001), platelets (56.1% vs. 12.8%, p < 0.001), and C-reactive protein (CRP) (70.6% vs. 41.7%, p = 0.002). A higher SII was also linked to hypoalbuminemia (38.5% vs. 7.6%, p = 0.001) and elevated CEA (52.9% vs. 31.5%, p < 0.026). The tumour-node-metastasis (TNM) stage IV exhibited a trend towards increased occurrences (63.6% vs. 38.0%, p = 0.053); however, the differences regarding T1–T2 (p = 0.167) and N0 (p = 0.379) were not statistically significant. The systemic immune-inflammation index effectively stratified systemic inflammatory parameters; nonetheless, it demonstrated weaker capacity in differentiating tumour stage or grade (p = 0.485).
Baseline and clinical characteristics of patients stratified by systemic inflammation response index cut-off
Patients with SIRI > 4.40 had fewer T1–T2 tumours (9.4% vs. 27.9%, p = 0.024) and a significant increase in stage IV disease (84.0% vs. 36.6%, p < 0.001) compared to those with SIRI ≤ 4.40. Unresectable tumours were more common (81.3% vs. 47.2%, p < 0.001), as was a family history of cancer (50.0% vs. 30.5%, p = 0.028). Inflammatory markers were significantly elevated, including WBC (71.9% vs. 10.4%, p < 0.001), platelets (34.4% vs. 17.3%, p < 0.020), and CRP (88.0% vs. 40.7%, p < 0.001). Elevated alkaline phosphatase (ALP) (76.0% vs. 51.0%, p = 0.018), AST (50.0% vs. 25.7%, p < 0.004), and CEA (57.7% vs. 31.7%, p = 0.009) also differed significantly, along with hypoalbuminemia (44.4% vs. 8.3%, p < 0.009).
Baseline and clinical characteristics of patients stratified by inflammatory benchmark index cut-off
Patients with an IBI ≤ 10.75 had fewer T1–T2 tumours (12.8% vs. 29.0%, p = 0.038), a higher proportion of stage IV disease (69.7% vs. 35.2%, p = 0.002), and more unresectable tumours (71.8% vs. 47.6%, p = 0.006) compared to those with an IBI > 10.75. Inflammation was significant, with elevated WBC (36.1% vs. 14.5%, p < 0.002) and CRP (100.0% vs. 34.9%, p < 0.001). Liver dysfunction was also more apparent, indicated by elevated AST (43.2% vs. 25.5%, p < 0.031), bilirubin (25.0% vs. 6.7%, p < 0.003), and ALP (82.6% vs. 49.7%, p = 0.003). The inflammatory benchmark index effectively stratified tumour stage and inflammatory mar-kers, demonstrating a notable inverse risk profile (Table 3).
Table 3
Baseline characteristics of patients stratified by inflammatory benchmark index cut-off (10.75) and associated p-values
| Characteristic | N | IBI ≤ 10.75, n = 39 (%) | IBI > 10.75, n = 169 (%) | p-value | |
|---|---|---|---|---|---|
| T1–T2 [22] | 208 | 5 (12.8) | 49 (29.0) | 0.038 | |
| N0 [22] | 208 | 6 (15.4) | 31 (18.3) | 0.663 | |
| TNM stage [22] | 178 | 0.002 | |||
| I–III | 10 (30.3) | 94 (64.8) | |||
| IV | 23 (69.7) | 51 (35.2) | |||
| Grading [22] | 208 | 0.151 | |||
| G1 | 3 (7.7) | 17 (10.1) | |||
| G2 | 14 (35.9) | 86 (50.9) | |||
| G3 | 6 (15.4) | 27 (16.0) | |||
| Gx | 16 (41.0) | 39 (23.1) | |||
| Pancreas locality/location | 208 | 0.414 | |||
| Head | 25 (64.1) | 111 (65.7) | |||
| Other | 14 (35.9) | 58 (34.3) | |||
| BMI [20] | 199 | 0.315 | |||
| > 23.51 | 21 (58.3) | 80 (49.1) | |||
| ≤ 23.51 | 15 (41.7) | 83 (50.9) | |||
| Age, median (IQR) | 208 | 65.0 (60.0–71.5) | 66.0 (61.0–70.0) | 0.536 | |
| Diabetes mellitus [28] | 207 | 10 (25.6) | 66 (39.3) | 0.111 | |
| Hypertension [29] | 206 | 15 (39.5) | 94 (56.0) | 0.066 | |
| Immune disease | 203 | 5 (13.2) | 21 (12.7) | 1.000 | |
| Current smoker | 185 | 13 (39.4) | 73 (48.0) | 0.367 | |
| Family history of cancer | 191 | 15 (44.1) | 52 (33.1) | 0.223 | |
| Unresectable [30] | 205 | 28 (71.8) | 79 (47.6) | 0.006 | |
| ALT [U/l] > 31.0 [31] | 281 | 59 (35.8) | 13 (35.1) | 0.943 | |
| AST [U/l] > 31.0 [31] | 281 | 42 (25.5) | 16 (43.2) | 0.031 | |
| Albumin [g/dl] ≤ 3.5 [32] | 105 | 3 (4.11) | 6 (50.0) | < 0.001 | |
| Total bilirubin [mg/dl] > 1.2 [33] | 280 | 11 (6.7) | 9 (25.0) | 0.003 | |
| ALP [U/l] > 104.0 [34] | 230 | 71 (49.7) | 19 (82.6) | 0.003 | |
| CRP [mg/l] > 5.0 [35] | 203 | 59 (34.9) | 39 (100.0) | < 0.001 | |
| CA 19-9 [IU/ml] > 37.0 [36] | 270 | 100 (60.6) | 28 (75.7) | 0.126 | |
| CEA [ng/ml] > 5.0 [37] | 234 | 44 (29.9) | 16 (53.3) | 0.014 | |
| Haemoglobin [g/dl] ≤ 11.0 [38] | 283 | 20 (11.8) | 9 (23.1) | 0.116 | |
| WBC [×103/µl] > 10.0 [12] | 283 | 24 (14.5) | 13 (36.1) | 0.002 | |
| Platelets [×103/µl] > 400.0 [39] | 283 | 34 (20.1) | 10 (25.6) | 0.447 | |
| SII > 1657.4 [24] | 283 | 21 (12.7) | 13 (36.1) | < 0.001 | |
| SIRI > 4.4 [23] | 202 | 12 (7.2) | 13 (36.1) | < 0.001 | |
[i] ALP – alkaline phosphatase, ALT – alanine aminotransferase, AST – aspartate aminotransferase, BMI – body mass index, CA 19-9 – carbohydrate antigen 19-9, CEA – carcinoembryonic antigen, CRP – C-reactive protein, IBI – inflammatory benchmark index, IQR – interquartile range, SII – systemic immune-inflammation index, SIRI – systemic inflammation response index, TNM – tumour-node-metastasis, WBC – white blood cell
Data presented as n (%) or median (IQR) unless otherwise specified.
P-values calculated using Pearson’s χ2 test, Fisher’s exact test, or Wilcoxon rank-sum test as appropriate.
P-values were established using the appropriate tests: Pearson’s χ2 test and Fisher’s exact test for categorical variables, and the Wilcoxon rank-sum test for continuous variables.
Discussion
Inflammation is closely related to the occurrence, development, and prognosis of tumours. This interplay of various immune cells, inflammatory cells, chemokines, and cytokines is recognized as a key characteristic of malignant neoplasms [40]. Given these findings, there is a growing focus on the inflammatory status of patients with PC and how inflammation affects mortality and prognosis. This study examined and compared the clinical and prognostic significance of three calculated pre-treatment inflammatory indices – SII, SIRI, and IBI in patients with PC.
Systemic immune-inflammation index combines platelets, neutrophils, and lymphocytes [24]. In SIRI, platelets convert to monocytes [23]. Inflammatory benchmark index encompasses all of them, with neutrophils, lymphocytes, platelets, and monocytes categorized by CRP concentration [25]. There is no consensus on the cut-off value for these indices. They have been studied in various patient cohorts with PC; nevertheless, our study is the first to compare these three indices and their prognostic value.
First introduced in 2016, SIRI integrates three critical leukocyte subtypes to provide a broader reflection of the tumour-host inflammatory environment [41]. In the meta-analysis by Shen and Zuo [23], which included 1160 patients, higher SIRI was associated with worse OS and PFS. Some studies identified a significant correlation between high levels of SIRI and SII, cancer location in the pancreatic head, and advanced TNM stage [42]. In our analysis, SIRI effectively stratified tumour stage, grade, and inflammation, reflecting an advanced disease burden. The pathophysiological basis lies in the pro-tumour functions of neutrophils and monocytes (such as promoting angiogenesis, aiding metastasis through tumour-associated macrophages, and suppressing lymphocyte-mediated immunity), while reduced lymphocytes indicate impaired anti- tumour surveillance [43].
Systemic immune-inflammation index combines two previously studied parameters: PLR and NLR. First, SII was examined as a prognostic indicator for the clinical outcomes of patients with hepatocellular carcinoma and small-cell lung cancer [24, 44]. A high SII indicates the combined effects of thrombocytosis and neutrophilia, which promote tumour progression through mechanisms such as angiogenesis, metastasis, and immune evasion. Conversely, lymphopenia signifies a diminished adaptive immune response, thereby impairing anti-tumour surveillance, for example, through decreased cytotoxic lymphocyte activity [45, 46]. A meta-analysis of the prognostic value of SII in 11 cohorts of patients with PC revealed that elevated SII was predictive of poor OS, recurrence-free survival (RFS), PFS, and DFS among patients of Asian ethnicity, in stages III–IV and recurrent disease, with a SII cut-off value of ≥ 900. Interestingly, no significant correlation was found between SII and several clinicopathological features. The authors suggested that this lack of association between SII and clinicopathological characteristics could have resulted from the limited sample size in each group [47].
Inflammatory benchmark index in PC was developed by Neumann et al. [25]. It includes CRP along with platelets, neutrophils, lymphocytes, and monocytes. Elevated plasma CRP levels have previously been linked to poor clinical outcomes in patients with PC. Numerous theories have been proposed to explain this relationship. One theory associates a higher tumour stage with increased systemic inflammation, marked by the secretion of cytokines and the release of tumour-degradation products, which elevates CRP production in the liver [48]. Another suggests that elevated CRP levels may foster tumorigenesis by both directly and indirectly activating protumorigenic pathways [49]. In our previous study conducted with patients who have PC and diabetes mellitus, a higher level of CRP was the strongest predictor of survival [50]. In the study by Neumann et al. [25], IBI was highly significant in both univariate and multivariate analyses of prognostic factors for OS in PC, independent of tumour stage and performance status. Our study confirmed the prognostic role of IBI. Inflammatory benchmark index predicted OS in both the adjuvant and palliative groups, alongside DFS and PFS. Moreover, IBI effectively stratified tumour stage, as patients with lower IBI counts had fewer T1–T2 tumours, more stage IV disease, and a higher rate of unresectable tumours at diagnosis. In the study conducted by Huang et al. [51], IBI was recognized as the most effective inflammatory index for predicting the prognosis of advanced gastric cancer treated with neoadjuvant chemotherapy in conjunction with immunotherapy. Furthermore, in the study by Aoyama et al. [52], IBI emerged as an independent prognostic factor for both OS and RFS in patients with esophageal cancer treated with curative intent. Population-level data from the National Health and Nutrition Examination Survey (a cohort of 14,835 participants from America) further demonstrated that each standard deviation increase in IBI was associated with a 23% higher risk of all-cause mortality and a 14% higher risk of cancer-specific mortality. Additionally, it enhanced risk stratification when integrated with traditional predictors [53].
Study limitations
This analysis has certain limitations. Selection bias may occur, as this was a single-centre, retrospective study. There are no agreed-upon cut-off values for the analysed indices. Most studies determine individual cut-off levels, demonstrating a significant prediction of survival; consequently, there is a wide range of cut-off values for these indices. A large, prospective, multicohort study should validate the optimal cut-off of SII, SIRI, and IBI and their prognostic value in clinical practice. Furthermore, the parameters analysed may easily change with the timing of the blood test, which further limits reliable patient stratification.
Conclusions
All analysed indices related to inflammation and immune response may serve as prognostic markers; however, further studies are imperative to ascertain their precise cut-off values. In our research, IBI exhibited a notably significant reduction of 65% in mortality, thereby highlighting the importance of CRP in patient stratification. An ongoing question pertains to the enhancement of the developed indices and whether indicators of malnutrition or hepatic impairment should be incorporated to elevate both sensitivity and specificity.






