





In recent years, the treatment of coronary artery diseases (CAD) has improved due to the advancements in percutaneous interventional techniques and the emergence of new intravascular imaging modalities. Nevertheless, severely calcified coronary lesions still present a significant challenge in percutaneous coronary intervention (PCI) procedures. Although drug-eluting stents (DES) are routinely used, their effectiveness depends on complete expansion, which is often limited in diffusely/severely calcified vessels and may lead to restenosis or in-stent thrombosis [1]. In such cases, the “leave-nothing-behind” strategy using drug-eluting balloons (DEB) offers a potential alternative. DEBs deliver antiproliferative agents directly to the vessel wall without leaving a permanent metallic scaffold, potentially reducing long-term complications associated with suboptimal stent expansion. DEB therapy, while initially validated for in-stent restenosis and small vessel disease, has recently been the subject of interest in the context of application to de novo lesions, including those with significant calcification [2].
A 77-year-old male was admitted for a complex PCI at a tertiary center following an unsuccessful attempt at angioplasty of the culprit lesion in non-ST-segment elevation myocardial infarction (NSTEMI). Coronary angiography revealed a severely calcified right coronary artery (RCA) (Figure 1 A) with a 99% stenosis and a proximal reference vessel diameter of 5.5 mm. His medical history is notable for heart failure with preserved ejection fraction, hyperlipidemia, hypertension and persistent atrial fibrillation. At baseline, the patient was receiving apixaban, eplerenone, nebivolol, dapagliflozin, perindopril, and indapamide. Intervention was conducted using a 7F Glidesheath Slender (Terumo, Tokyo, Japan) introducer sheath and a 7FAR2.0 (Medtronic, Minneapolis, MN, USA) guiding catheter via the right radial artery approach. Runthrough NS (Terumo, Tokyo, Japan), Sion Blue ES (Asahi Intecc, Aichi, Japan), and Shun R (Shunmei Medical Co., Ltd, Shenzhen, China) guidewires were used during the procedure. The Runthrough NS served as the primary workhouse wire while Sion Blue ES and Shun R were used for crossing the calcium lesion and facilitating atherectomy. Parallel wiring was not performed; instead, multiple techniques were employed to ensure adequate support throughout the procedure. An attempt to predilate the lesion with a 2.0 × 15 mm balloon at 18 atm resulted in a balloon rupture. Subsequently, a 2.5 × 15 mm non-compliant balloon was used at 18 atm. As the predilatation was insufficient, rotational atherectomy of the proximal RCA was conducted using a 1.5 mm RotaPro burr over a Rotawire Floppy (Boston Scientific, Marlborough, MA, USA) guidewire (Figure 1 B). Post-atherectomy intravascular ultrasound (IVUS) demonstrated a minimal lumen area of 3.3 mm2 and a circumferential calcium arc of 360°.
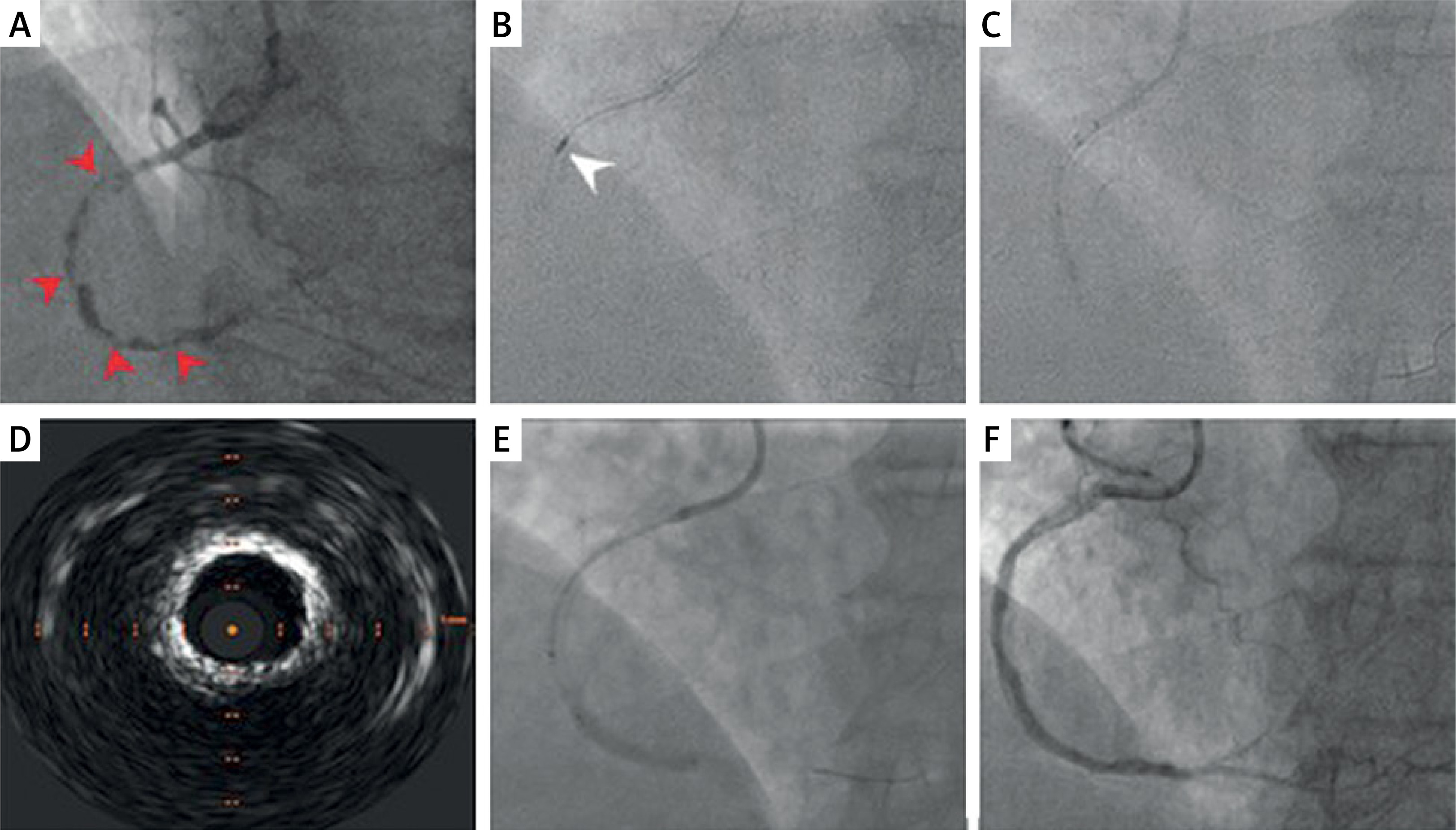
Figure 1
All coronary angiograms are presented in the 30° left anterior oblique (LAO) projection. A – Initial angiogram of the right coronary artery (RCA) demonstrating 99% proximal stenosis with diffuse lesions along its length (red arrowheads). B – Rotational atherectomy of the proximal RCA segment (white arrowhead). C – Intravascular lithotripsy. D – Intravascular ultrasound (IVUS) demonstrating a circumferential (360°) calcium ring with a rigid, non-fragmented atherosclerotic plaque, precluding stent implantation. E – Drug-eluting balloon angioplasty of the distal RCA segment. F – Final angiogram showing restored TIMI 3 flow and reduction of proximal stenosis to 30%
Predilatation was then performed using non-compliant balloons: 3.0 × 20 mm inflated to 20 atm, followed by 3.5 × 20 mm inflated to 18 atm to facilitate positioning of the lithotripsy device. Intravascular lithotripsy was performed using Shockwave C2+ 3.5 × 12 mm system (Shockwave Medical, Santa Clara, CA, USA), delivered with an assistance of Guidezilla II (Boston Scientific, Marlborough, MA, USA) guide extension (Figure 1 C). The vessel was then inflated using an OPN (Medtronic, Minneapolis, MN, USA) super-high pressure catheter balloon 3.5 × 20 mm at 30 atm. IVUS revealed a satisfactory lumen gain but inadequate plaque modification, characterized by the absence of calcium fractures (Figure 1 D) and failure to achieve full balloon expansion. Due to the 360° circumferential calcium arc, a stent was avoided, and a DEB was employed to prevent underexpansion while ensuring effective long-term antiproliferative effect. The drug-eluting balloon angioplasty was performed distally using a SeQuent Please NEO (B. Braun Melsungen AG, Melsungen, Germany) 4.0 × 30 mm balloon at 10 atm for 60 s (Figure 1 E), followed by a proximal inflation with a 4.0 × 40 mm balloon with 10 atm for 60 s. Afterwards, a slow-flow phenomenon in the revascularized RCA was observed (Figure 1 F). This transient distal perfusion impairment likely resulted from a combination of embolization of plaque fragments, microvascular spasm, and endothelial injury due to calcium modification. Although slow flow is well documented after atherectomy and complex PCI, its occurrence after drug-eluting balloon use in heavily calcified lesions is uncommon but plausible given the extent of circumferential calcification. Preventive strategies for such high-risk lesions involve imaging-guided lesion preparation, cautious application of calcium-modifying tools, and readiness to administer intracoronary vasodilators as well as preprocedural initiation of high-intensity lipid-lowering therapy [3]. Consequently, a 200 µg bolus of sodium nitroprusside was administered intracoronary, resulting in a TIMI 3 grade flow. Following the intervention, the RCA stenosis decreased to 30% from 99% at baseline. Post-procedurally, the patient developed an allergic reaction to contrast media which was treated with dexamethasone and clemastine. At discharge, the patient, already on apixaban, was prescribed dual antiplatelet therapy with aspirin 75 mg and clopidogrel 75 mg daily for 1 month, followed by clopidogrel alone for the next 6 months. The postprocedural period was uneventful and at 6-month follow-up, the patient remained asymptomatic, with no recurrence of angina.
This case demonstrates an uncommon clinical setting in which the combined use of the various calcium modification techniques was insufficient to achieve sufficient plaque modification for optimal stent insertion and expansion. In such patients, the “leave-nothing-behind” strategy is a viable alternative approach, which may potentially lead to more favorable long-term outcomes [4].