Vasospastic angina, along with coronary microvascular dysfunction, is one of the causes of resting chest pain in patients without significant epicardial coronary artery stenosis. Coronary artery spasm, which may involve both epicardial vessels and the microvasculature, can be focal or diffuse. This leads to myocardial ischemia, which may result in acute coronary syndrome, ventricular arrhythmias, syncope, and sudden cardiac arrest.
A 44-year-old male patient, an active smoker, with hypertension and type 2 diabetes, previously diagnosed with ventricular arrhythmia, was admitted to the hospital after three episodes of syncope preceded by chest pain. Ten months earlier, the patient had suffered from a lateral wall ST-elevation myocardial infarction, treated with primary angioplasty with stent implantation of the circumflex branch (Cx). Echocardiography revealed normal heart chamber dimensions, no significant valvular defects, and some regional wall motion abnormalities – akinesia of the mid and basal segments of the posterior wall and hypokinesia of the basal segment of the lateral wall, with preserved ejection fraction (62%). During continuous Holter-ECG monitoring, another episode of typical chest pain occurred in the early morning hours and resolved after short-acting nitrates. ECG showed transient ST-segment elevation and ventricular bigeminy (Figure 1 A). The patient was referred for an urgent coronary angiography, which initially showed borderline narrowing of the left main coronary artery and patent stent in Cx (Figure 1 B). During subsequent radiograms, the patient reported severe chest pain with ECG showing ST-segment elevation and ventricular arrhythmia, and angiography confirmed spasm of the left main coronary artery (LMCA) (Figure 1 C). After intracoronary administration of 300 ug of nitroglycerin, the pain subsided gradually, ST-segment normalized, and arrhythmia resolved. High-definition intravascular ultrasound (HD IVUS) revealed no significant changes, like plaque rupture or ulceration, thrombus or dissection but only intimal thickening in the LMCA and left anterior descending artery (Figure 1 D). Prinzmetal’s angina was diagnosed. Bisoprolol was discontinued, and treatment with verapamil 120 mg twice daily and long-acting nitrates was initiated. The patient was advised to stop smoking and to control traditional risk factors. According to the Coronary Artery Vasospastic Disorders Summit criteria, vasospastic angina can be diagnosed if an unprovoked chest pain rapidly resolves with nitrates and is accompanied by transient ischemic ECG changes (ST-segment elevation or depression ≥ 0.1 mV, new negative U wave) or coronary artery spasm, with ≥ 90% vessel lumen narrowing [1]. Besides smoking, most classical coronary artery disease risk factors appear unrelated to vasospastic angina prevalence [2]. Spasm of the LMCA is a rarely observed and described form of vasospastic angina in the literature. It can occur either spontaneously or iatrogenically, most commonly provoked by a catheter intubation [3]. It is crucial to distinguish LMCA spasm from atherosclerotic changes in order to avoid unnecessary coronary artery bypass grafting and to implement appropriate pharmacotherapy. Intravascular ultrasound allows to exclude the presence of significant atherosclerotic plaque and potential causes of acute coronary syndromes [4].
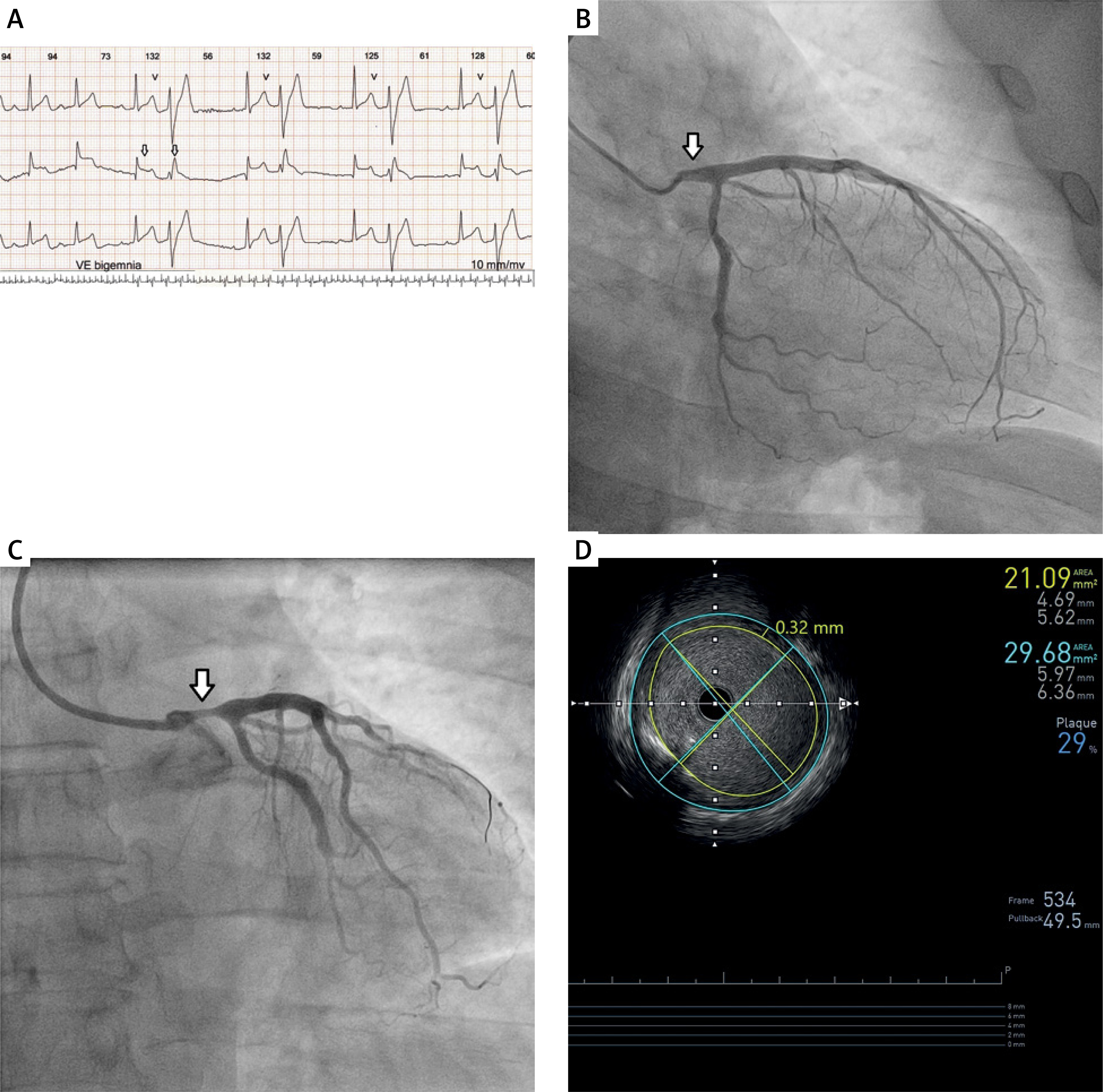
Figure 1
A – Continuous Holter-ECG monitoring during an episode of typical chest pain showing transient ST-segment elevation and ventricular bigeminy. B – Baseline coronary angiography showing borderline narrowing of the left main coronary artery. C – Angiography during chest pain confirming spasm of the left main coronary artery (LMCA). D – High-resolution intravascular ultrasound indicating minor wall changes in the LMCA and left anterior descending artery