
Introduction
Patients with untreated significant unprotected left main coronary artery (ULM) disease have a poor prognosis and revascularization with coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) is indicated [1]. Randomized trials comparing CABG and ULM PCI showed no significant difference in the risk of death even during extended 10-year observational periods [2, 3]. It is important to notice, however, that patients enrolled in randomized trials are highly selected with low or intermediate SYNTAX score and suitable for both revascularization strategies. Accordingly, long-term survival of all-comer patient population with significant ULM stenosis may be different as reported in randomized trials and may vary according to revascularization strategy.
The aim of our study was therefore to investigate a long-term survival in consecutive patients with significant ULM disease undergoing one of the revascularization procedures who presented to a single cardiovascular centre.
Methods
This was a retrospective observational study which enrolled consecutive patients with ≥ 50% ULM stenosis undergoing either isolated CABG or ULM PCI at the international cardiovascular centre MC Medicor, Izola (Slovenia). A decision for CABG or ULM PCI was made by the institutional heart team in agreement with patient preferences. All patients received a comprehensive explanation of the selected revascularization procedure and signed written informed consent for the procedure. CABG was performed by one of the three high-volume cardiac surgeons who worked in MC Medicor in different time periods. All ULM PCI procedures were performed by a single high-volume interventional cardiologist with extensive experience in ULM PCI with cumulatively > 300 procedures at different institutions. Patient data were obtained from the institutional registry of cardiovascular interventions which was approved by the Slovenian National Ethic Committee (Number 93/11/12).
The date of eventual patient death was obtained from the “National BIRPIS” system using the patient’s health insurance card number. Numerical data are presented as mean values with standard deviations or median values with interquartile range (IQR). Categorical data are presented as absolute numbers and percentages. Numerical variables were compared with unpaired t-test or Mann-Whitney U test in case of abnormal distribution. Categorical variables were compared with c2 test or Fisher’s exact test. The likelihood of 5- and 10-year survival was estimated with Kaplan-Meier method. Multivariable Cox proportional hazards regression analysis was performed to adjust for baseline differences between groups including age, sex, logistic EuroScore and presence of multivessel disease. A p-value of less than 0.05 was considered as significant.
Results
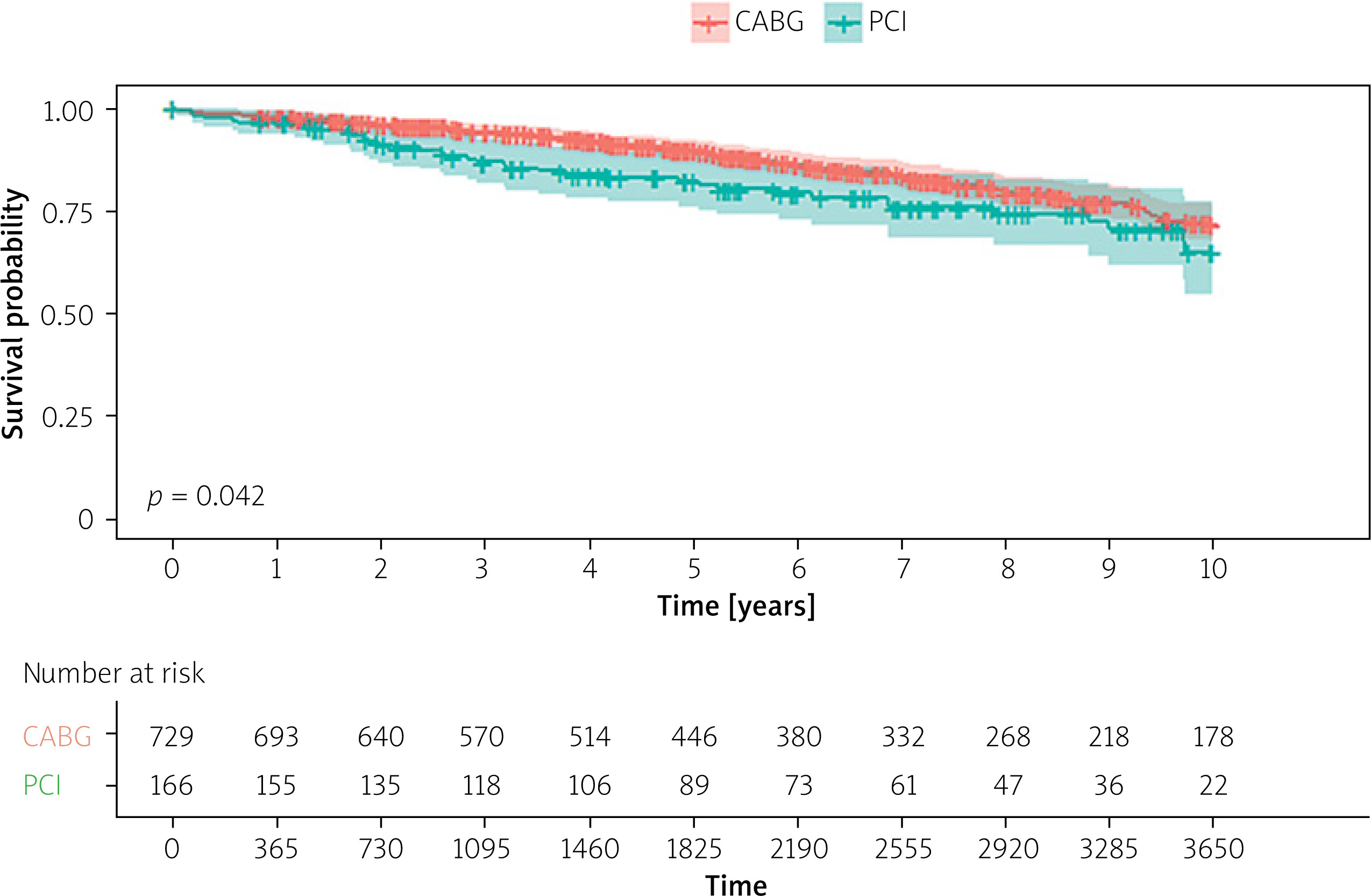
From February 2006 to October 2023, among 895 consecutive patients presenting with significant ULM stenosis to MC Medicor, 729 underwent CABG (81.5%) and 166 ULM PCI (18.5%). Patients undergoing CABG were significantly younger (67 vs. 70 years), more often men (84% vs. 69%) and presented less frequently with acute coronary syndrome (0% vs. 13%) (Table I). Multivessel disease was present more often in CABG patients (80% versus 32%) who had lower logistic EuroScore compared to patients undergoing ULM PCI (4.4 vs. 5.6).
Table I
Features of consecutive patients with unprotected left main stenosis undergoing coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) at MC Medicor Izola (Slovenia) between 2006–2023
Patients undergoing CABG received 1-5 grafts (3.0 ±1.6) with the left mammary artery to the left descending coronary artery as a default strategy. In patients undergoing ULM PCI, drug eluting stents (DES) were implanted in 98%. Provisional stenting was used as a default strategy. Wire recrossing to the left circumflex artery and balloon kissing was performed in 28%. The two-stent technique including “T-TAP” or culotte, was used in 11%. Good angiographic results were documented in 100%. Intravascular imaging and functional assessment were used in 15.6%.
The median follow-up for patients undergoing CABG and PCI was 2829 days (25th and 75th IQR 1634–4358 days) and 2622 days (25th and 75th IQR 1558–3639 days), respectively (p = 0.154). While 30-day mortality was comparable between CABG and ULM PCI patients (0.8% vs. 0.6%), mortality at 5 years (10.2% vs. 17.9%; p = 0.005) and 10 years (28.4% vs. 35.1%; p = 0.042) was significantly lower in CABG patients (Figure 1). After multivariable adjustment, revascularization strategy remained independently associated with long-term mortality (hazard ratio = [HR] 1.55; 95% confidence interval [CI]: 1.05–2.28; p = 0.028).
Discussion
Our study demonstrated that CABG, which was performed in more than 80% of our patients, remains the predominant revascularization strategy for treatment of significant ULM disease in all-comer patient population. Although percentage of CABG is rather high compared to PCI, our finding is in accordance with recently published results of the large SWEDEHEART registry in which 84% of patients had CABG as a revascularization strategy [4]. On the other hand, it is important to notice that the annual number and percentage of ULM PCI compared to the total number of revascularization procedures is gradually increasing which may change predominance of CABG as the preferred revascularization strategy in ULM patients in the near future [5].
We demonstrated that CABG was, compared to ULM PCI, associated with decreased 5-year and 10-year mortality. This finding, which is in contrast with randomized trials [1–3], may be, at least in part, explained by the fact that our patients undergoing ULM PCI were older, had more comorbidities, presented more often with acute coronary syndrome and were therefore often rejected for CABG. Although the difference in long-term survival persisted after multivariable adjustment, it is important to emphasize that ULM patients disqualified from CABG have, despite good procedural results, increased long-term mortality after PCI [6].
Long-term mortality in our patients, which was the primary study endpoint, is in accordance with the SWEDEHEART registry in which 9364 patients undergoing CABG had significantly lower 5-year mortality (8.5% vs. 22.2%) and 10-year mortality (15.5% vs. 35.5%) than 1733 patients treated by ULM PCI [3]. We further compared long-term mortality between MC Medicor and SWEDEHEART registry according to revascularization strategy. While our CABG mortality at 5 years was comparable to that of SWEDEHEART (10.2% vs. 8.5%), it significantly increased at 10 years (28.4% vs. 15.5%). We do not have a sound explanation for this finding which may be related to more frequent complete arterial revascularization or better secondary prevention and medical therapy in Sweden compared to Slovenia. Unfortunately, we do not have data such as discharge medication and adherence to secondary prevention to support this hypothesis. On the other hand, our ULM PCI mortality at 5 years (16.2% vs. 19.2%) and 10 years (35.1% vs. 35.5%) was very comparable to that of SWEDEHEART despite rather limited use of intravascular physiology and imaging in our patients. Very low penetration of intravascular imaging and physiology according to worldwide standards in our patients is mainly related to the fact that these methods are, also to our surprise, still not reimbursed in Slovenia even for ULM PCI. We can only speculate that long-term survival of our PCI cohort would have been improved if intravascular imaging was used more often [5].
Our results should be obviously interpreted in view of the retrospective study design which did not allow us to collect more detailed patient demographic characteristics, angiographic features including SYNTAX score and procedural characteristics related to PCI. Importantly, if two-stent technique was necessary, we used “T-TAP” or double-kissing culotte technique which might be superior to double kissing crush technique in terms of target lesion revascularization [7]. Furthermore, only mortality rather than all components of major adverse cardiac events was used as a primary study endpoint. We are also aware that these results are valid only for our institution and particular physicians performing ULM revascularization procedures. We also acknowledge that the number of ULM PCI patients is rather small which represents another important limitation of our study.
In conclusion, our study underscores the fact that randomized clinical trials performed in carefully selected patients may not reflect everyday clinical practice and outcomes. It also emphasizes the importance of continuous monitoring of institutional outcomes of invasive cardiovascular procedures with results incorporated in the decision-making process of the institutional heart team and patient informed consent.







