
The transradial approach is the preferred access for coronary and peripheral interventions, offering reduced bleeding risk and superior patient comfort compared with femoral access [1]. Vascular complications are rare; the incidence of radial artery pseudoaneurysm (RAP) is estimated at 0.08–0.6% [2]. The predisposing factors include multiple puncture attempts, anticoagulation, local infection, large sheath size, and inadequate hemostasis, typically due to insufficient compression, off-center device placement, premature deflation, or early wrist mobilization [3]. Over the past decade, our center reported 11 cases among 13,819 radial artery cannulations (incidence 0.08%), most of which were diagnosed early and managed conservatively. The following 2 cases illustrate extremely rare, late-onset presentations of this complication.
Case 1. An 82-year-old woman underwent staged percutaneous coronary interventions (PCI) via both radial arteries using 6F systems for symptomatic two-vessel coronary artery disease. Hemostasis was achieved after each procedure using a pneumatic compression band for 3–4 h, with compression adjusted according to the reverse Barbeau test, as per our cath lab protocol. The vascular access sites were appropriately healed at discharge. Two weeks after the second procedure, the patient developed right wrist pain accompanied by a progressively enlarging nodule. She did not seek medical attention until 3 months later, when a 41 × 29 × 20 mm pulsatile mass was identified. Duplex ultrasonography demonstrated a pseudoaneurysm of the right radial artery. The surgical excision was performed as the first-choice treatment due to the large size of the lesion, providing arterial patency and an excellent cosmetic result (Figure 1 A).
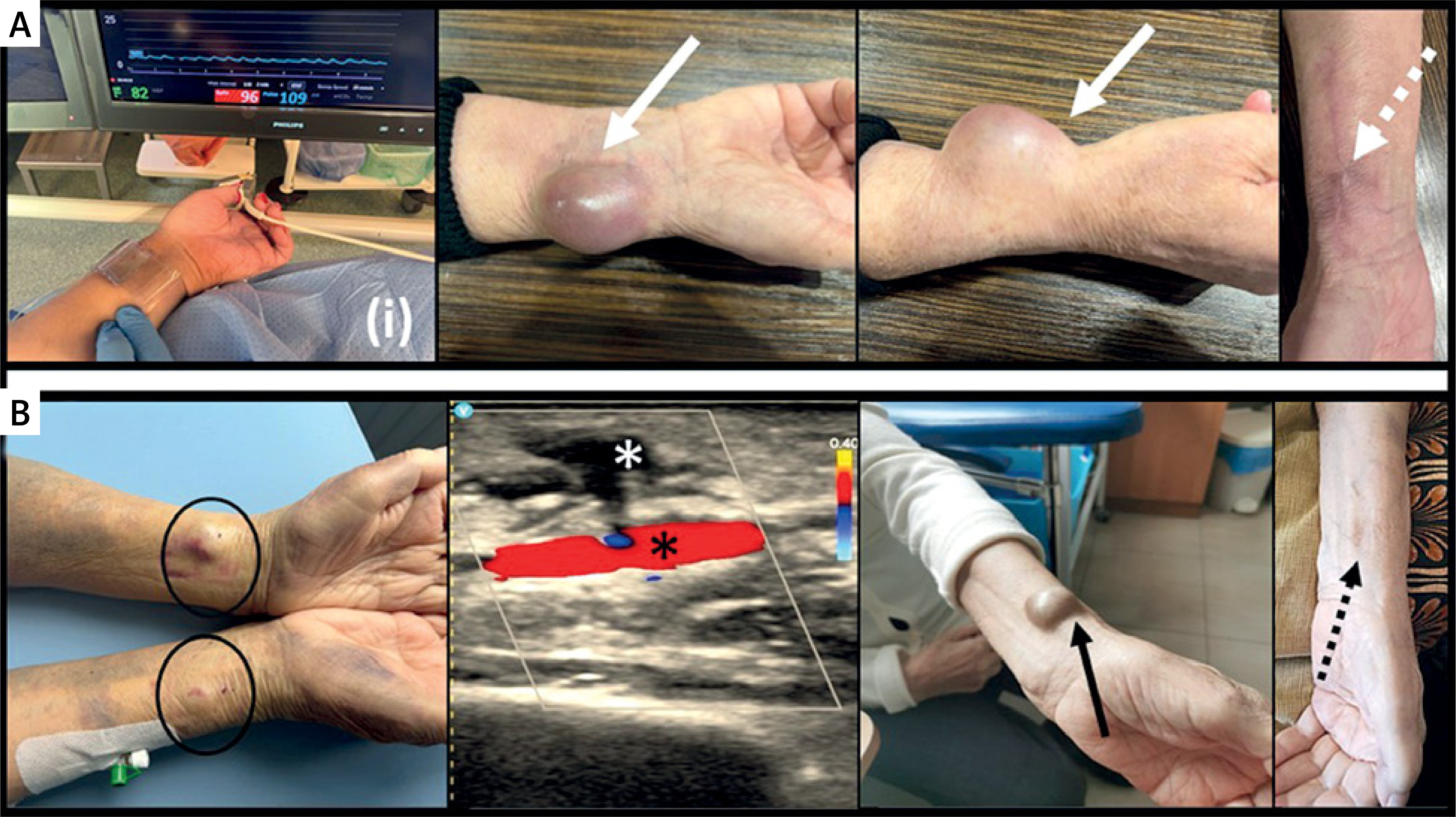
Figure 1
A - Despite adequate reverse Barbeau test-guided hemostasis ((i)) and no local vascular complications at discharge, a large right radial artery pseudoaneurysm occurred at 3 months post-PCI (solid white arrow), and postoperative result was provided with preserved radial pulse and a small residual scar (dashed white arrow). B – Bilateral radial artery pseudoaneurysms (black circle), successfully treated with 24 h of the prolonged local compression, showing no flow communication between the radial artery (black star) and the thrombosed pseudoaneurysm sac (white star) on duplex ultrasound, but with recurrence in the right forearm after 5 weeks (black solid arrow), effectively managed with the surgical intervention (black dashed arrow)
Case 2. An 89-year-old woman underwent staged PCI within a 2-day interval for non-ST-segment elevation myocardial infarction. Both procedures were performed via the radial arteries using 6F sheaths, with hemostasis achieved by compression, as in Case 1. Within several hours after removal of the compression bands, small bilateral pseudoaneurysms developed. As neither targeted ultrasound-guided compression nor 6-hour compression was effective, the patient underwent 24 h of pneumatic compression with reverse Barbeau-guided patency monitoring, achieving successful thrombosis of the pseudoaneurysm sac confirmed by follow-up ultrasonography. However, at 5 weeks, a 27 × 25 × 15 mm mass reappeared at the right wrist. Ultrasonography confirmed a large pseudoaneurysm that required surgical repair, resulting in a good vascular and cosmetic outcome (Figure 1 B).
A pulsatile, painful swelling at the puncture site should raise suspicion of RAP, confirmed by duplex ultrasonography. Most cases respond to the prolonged compression, but large or complicated lesions require surgery. Thrombin injection is not recommended due to the risk of embolization through short-neck pseudoaneurysms [4].
Both patients were elderly, suggesting that vascular fragility may have been a contributing factor. It should be emphasized that, even with safety-based cannulation, pseudoaneurysms may occur unpredictably, sometimes with delayed onset, even if no vascular complications were noted at the access site during hospitalization. Ultrasound-guided access, careful hemostasis, and trained post-procedural care are essential to minimize the risk. Patients should be informed of potential delayed complications and advised on early reporting of local symptoms.
Radial artery pseudoaneurysm remains a rare but clinically significant complication of transradial access. Early recognition, appropriate management, and vigilant follow-up ensure favorable outcomes.







