
A 55-year-old man presented to a district hospital with an inferolateral ST-elevation myocardial infarction (STEMI). As transfer for primary percutaneous coronary intervention (PPCI) within 120 min was not feasible, he was thrombolysed with tenecteplase. Thrombolysis with tenecteplase was unsuccessful, and he was subsequently transferred to our center for rescue percutaneous coronary intervention.
Emergency coronary angiography via the right radial artery showed an atheromatous but unobstructed left coronary system. The right coronary artery (RCA) demonstrated diffuse ectasia with a high thrombus burden in the proximal and mid segments resulting in TIMI grade 1 flow. Distal occlusion was noted just proximal to the crux, within an area of marked ectasia (Figure 1 A).
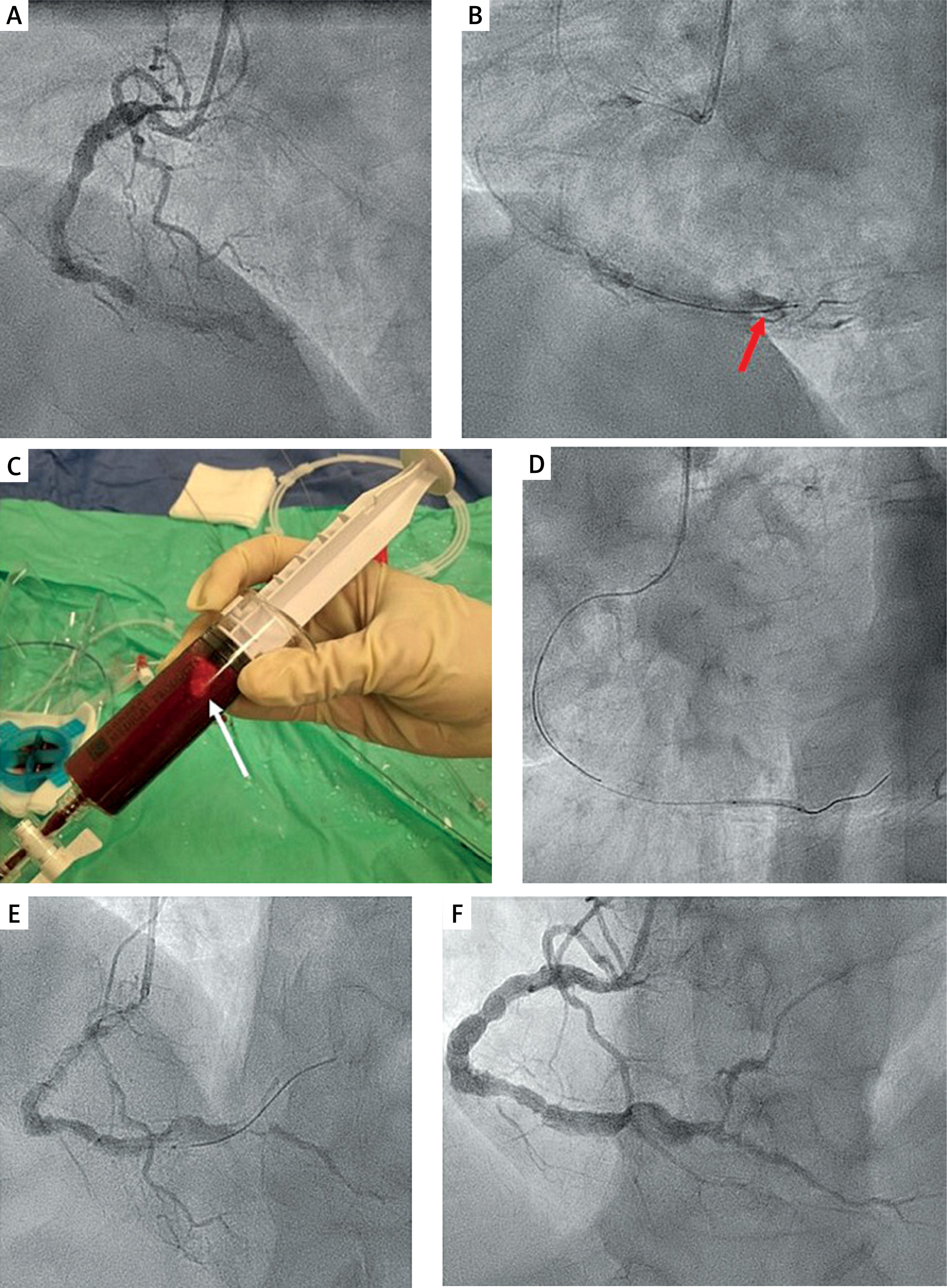
Figure 1
A – Coronary angiogram, left anterior oblique (LAO) view of the right coronary artery (RCA) demonstrates diffuse ectasia with a high thrombus burden and distal occlusion. B – The guidewire tip is located at the site of occlusion where a large thrombus is clearly visualized (red arrow). C – Large white thrombus particle observed in the aspiration syringe (white arrow). D – Balloon dilatation with a 2.0 × 20 mm semi-compliant balloon in the posterior descending artery. E – Angiographic view following dilatation in the posterolateral branch. F – Repeat coronary angiography 7 days later revealed improved angiographic appearance and TIMI 3 flow
A workhorse guidewire was advanced, although lesion crossing was initially difficult (Figure 1 B). Two thrombus aspiration sessions using a 6 Fr Thrombuster II (Kaneka Corporation, Osaka, Japan) device retrieved large white thrombus fragments (Figure 1 C). Subsequent administration of intracoronary tirofiban led to mild angiographic improvement. A 2.0 × 20 mm semi-compliant balloon was then used to support lesion crossing. The guidewire entered peripheral RCA branches, partially restoring flow (Figures 1 D, E). Balloon dilatations were subsequently performed with the 2.0 × 20 mm semi-compliant balloon in the posterior descending artery and posterolateral branch. Given the resolution of ST-segment elevation and a significant mismatch between the ectatic RCA and its distal branches, stenting was deferred. TIMI 2 flow was achieved in the RCA and its distal branches and the patient’s chest pain resolved.
The patient was admitted to the Coronary Care Unit on quadruple antithrombotic therapy (aspirin, ticagrelor, tirofiban infusion for 48 h, and a therapeutic dose of enoxaparin) without bleeding complications. Transthoracic echocardiography showed preserved left ventricular systolic function.
Repeat coronary angiography on day seven showed TIMI 3 flow throughout the RCA and its branches (Figure 1 F). Given the diffuse atherosclerotic pattern and the presence of diffuse ectasia, no further intervention was attempted. The patient was discharged on dual antiplatelet therapy with acetylsalicylic acid and ticagrelor. At 3-month follow-up, he remained asymptomatic, and a single-photon emission computed tomography scan revealed less than 5% of myocardial ischemia in the inferior wall.
Coronary artery aneurysms and coronary ectasia are found in up to 5% of patients undergoing coronary angiography [1]. This case highlights the challenges of managing STEMI in the presence of coronary artery ectasia and a high thrombus burden. Coronary ectasia patients with STEMI have higher rates of PCI failure and no-reflow due to an increased risk of distal embolization and difficulty in stenting [2]. This often necessitates a conservative or staged approach along with intensive antithrombotic therapy. A strategy involving initial undersized stenting followed by delayed intravascular ultrasound (IVUS) optimization to reduce embolization during the acute phase has been described for STEMI patients with a high thrombus burden [3]. Pharmacological management is fundamental for patients with coronary artery ectasia. Dual antiplatelet therapy is the most effective long-term treatment in the prevention of major adverse cardiovascular events in patients with coronary artery ectasia according to a recent meta-analysis [4].







