
Spontaneous isolated dissection of visceral arteries, including the celiac or superior mesenteric arteries (SMA), without associated aortic dissection, has been considered a rare clinical entity. However, reports of spontaneous isolated SMA dissection have recently increased with the advancement in computed tomography (CT) resolution [1, 2]. In contrast, isolated common hepatic artery dissection remains extremely rare, and its pathogenesis, natural course, optimal management, and prognosis are not well understood.
A 63-year-old man with a history of hypertension, diabetes mellitus, gastric ulcer, and chronic obstructive pulmonary disease presented with sudden onset epigastric pain persisting for more than 1 h following a bath, accompanied by cold sweat. He had been diagnosed with SMA dissection which was incidentally detected on CT and managed conservatively 2 years ago. There was no family history of aortic dissection or connective tissue disease, including Marfan syndrome or Ehlers-Danlos syndrome.
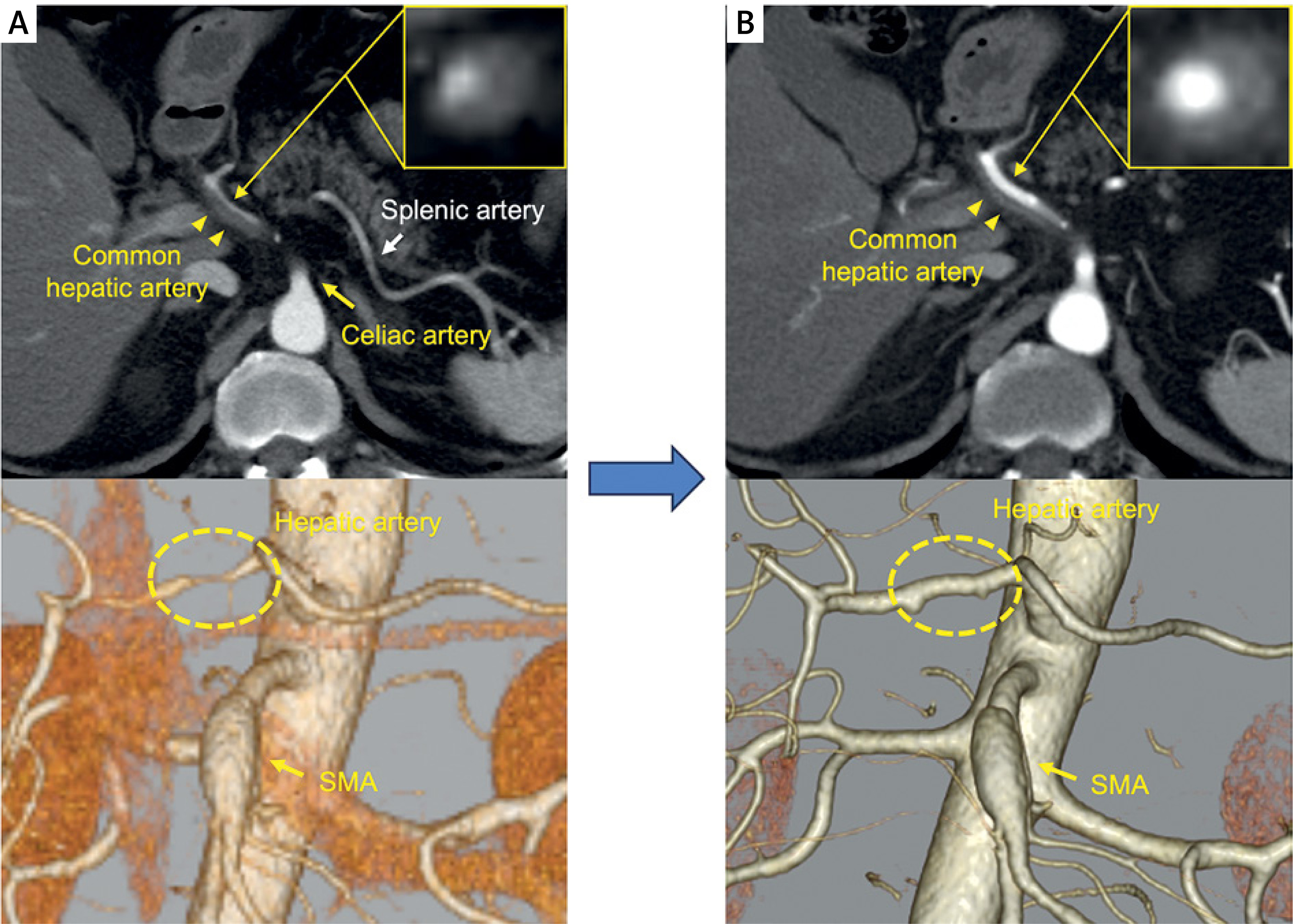
Contrast-enhanced CT showed dissection of the common hepatic artery with thrombosis in the false lumen (Figure 1 A). There were no dissections in the celiac and splenic arteries, and no significant changes in the SMA compared with findings from 2 years earlier. The patient was diagnosed with spontaneous isolated common hepatic artery dissection and was admitted for pain control and antihypertensive therapy, because peritoneal irritation signs or another complication was not detected. Follow-up contrast-enhanced CT on the fourth hospital day showed regression of the thrombus within the false lumen (Figure 1 B). The patient resumed oral intake and rehabilitation without recurrence of symptoms, and his blood pressure remained well-controlled. On the 12th hospital day, he was discharged without any complications.
Figure 1
Contrast-enhanced computed tomography (CT) findings. A – Contrast-enhanced abdominal CT on admission detected a dissection of the common hepatic artery with thrombosis in the false lumen (yellow arrowheads), and narrowing of the lumen in the short-axis view. No dissection was observed in the celiac artery (yellow arrow) and the splenic artery (white arrow). Three-dimensional CT showed narrowing of the hepatic artery (yellow dotted circle). No significant changes were noted in the superior mesenteric artery (SMA) compared to the previous imaging. B – Compared to the admission CT, regression of thrombus in the false lumen and improvement of stenosis in the common hepatic artery were observed on the fourth hospital day
The SMA and celiac artery are the most commonly affected visceral arteries, with isolated common hepatic artery dissection being exceptionally rare [3]. In the present case, a dissection of the common hepatic artery occurred during conservative follow-up for SMA dissection, making this case particularly noteworthy. Park et al. reported that over 70% of SMA dissection cases managed conservatively had no recurrence of symptoms [4]. However, complete remodeling in type IIa SMA dissection is observed in only 6.5% of cases [4]. Our case presented with the dissection of SMA with patency of the true and false lumen that is “type IIa”, therefore careful follow-up was required.
To the best of our knowledge, this is the first report of spontaneous isolated common hepatic artery dissection that occurred during conservative follow-up for SMA dissection. A previous study involving 46 patients with spontaneous isolated SMA dissection managed conservatively reported no progression or new dissections on follow-up CT angiography [4]. However, our case developed a new dissection despite conservative management, and this highlights that in patients undergoing conservative therapy for visceral arteries dissection, continuous monitoring and strict blood pressure control are essential. Guidelines for the management of aortic dissection recommend achieving a target blood pressure of < 130/80 mm Hg. However, this is a recurrent case involving two vessels; therefore, more intensive management might be required. CT follow-up should be scheduled at 6–12 months, depending on the patient’s symptoms.







