





A 30-year-old female with resistant arterial hypertension presented to the Department of Cardiology for clinical evaluation. Elevated blood pressure was first diagnosed 2 years before, during pregnancy and persisted after the delivery. On physical examination, she presented with diastolic murmur over the right sternal border. Transthoracic echocardiography revealed bicuspid aortic valve with mild insufficiency and dilatation of the aortic root. Computed tomography angiography (CTA) was performed for complete assessment of the aneurysm and revealed aortic isthmic atresia with extensive collateral circulation (Figure 1 A). The patient was qualified for percutaneous repair.
Figure 1
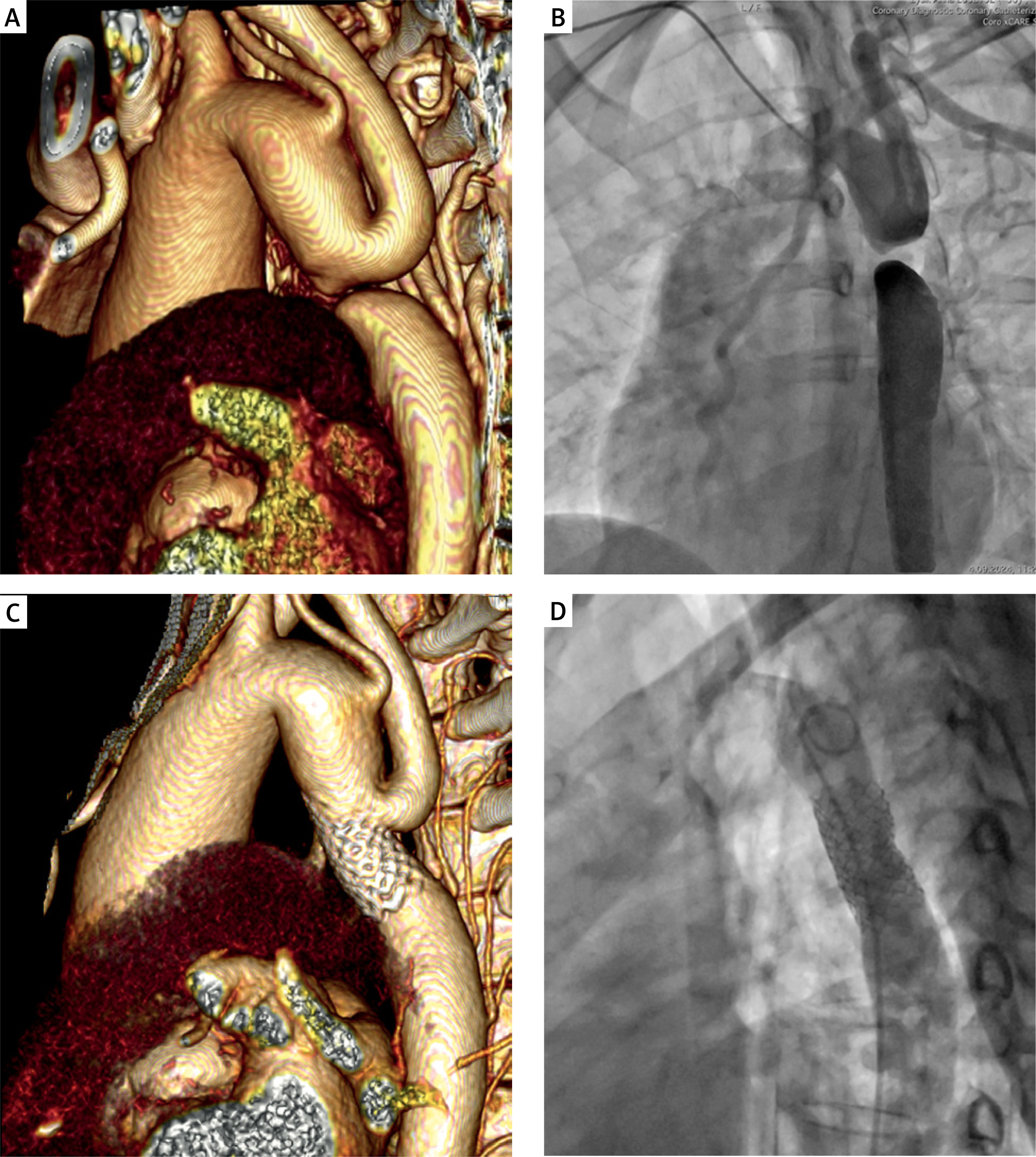
A – A 3D reconstruction of computed tomography angiography showing aortic atresia. B – Contrast administered to the region of aortic isthmus simultaneously from the antegrade and retrograde approach – there is no continuity between the aortic arch and descending aorta. C – A 3D reconstruction of computed tomography angiography showing the descending aorta reconstructed with a covered stent. D – The patient’s aorta after the 2nd intervention – a picture from classic angiography
Using an ante grade approach (right radial access) a pigtail catheter was introduced to the aortic arch (AA). Aortic atresia was confirmed with angiography (Figure 1 B). Communication between AA and descending aorta (Aodesc) was obtained from an antegrade approach, with a puncture of the sharp end of coronary guidewire. Subsequently, using a vascular loop technique, and dilatation with a coronary balloon, extra stiff guidewire was introduced through the patient’s radial artery to Aodesc, and evacuated via the right femoral artery. Finally, the site of atresia was secured and dilated by a covered stent (Bentley BeGraft 12 × 39 mm) implanted from a retrograde approach. In direct assessment, no pressure gradient through stent was recorded. The patient was discharged on the 3rd day post intervention in good condition. Satisfactory outcome was confirmed with a CTA (Figure 1 C). On 2-month follow-up, the patient remained normotensive without medications. As there was a peak systolic gradient of 50 mm Hg measured by transesophageal echocardiography (TEE), we performed percutaneous re-dilatation of the stent with an excellent result (Figure 1 D).
Aortic atresia is an extreme form of aortic coarctation. Patients’ survival is only possible thanks to collateral circulation that supplies the lower part of the body [1]. Adults with this rare heart defect can present with hypertension, headaches, nosebleeds, intermittent claudication or coronary arterial disease at a young age. Majority of them have concomitant bicuspid aortic valve, which brings forward the diagnosis.
In the last three decades, several cases of percutaneous repair have been reported [1–3]. So far, it appears a safe and cost-effective alternative for a classical, surgical approach. Whereas in the treatment of neonatal cases of aortic coarctation, surgical repair remains a method of choice, it is difficultly feasible with difficulty in adults due to limited mobility of tissues. Additionally, presence of extensive collateral circulation poses a high risk of bleeding and thromboembolic complications during anatomical repair [4].
Prior case reports illustrate that endovascular recanalization of the atretic isthmus can be successfully performed using three methods: stiff end wire, transseptal needle and radiofrequency ablation. In the biggest case series of 19 patients published by Chessa et al. [2], only 2 patients developed complications and 1 patient died, which is an excellent result.
Potential complications of this procedure include dissection or perforation of the recanalized aorta, long-term restenosis of the implanted stent [1], as well as local complications associated with arterial puncture. However, they appear infrequent as compared to the risks of open-heart surgery, and the patient’s full recovery after percutaneous angioplasty remains considerably shorter.
However, endovascular repair has its certain limitations, which make it infeasible in particular patients. First, as the stent needs adequate landing zones for its proximal and distal ends, dilatation of aorta proximally and distally to the atretic segment, poses a risk of stent sliding. Second, covered stent expanded in the isthmus can collide with the left subclavian artery. The case implies that small distance from the aortic branch does not have to be the reason for disqualification from endovascular repair.