





Atrial fibrillation (AF), being one of the most common arrhythmias, constitutes a major public health burden. Treatment is crucial due to complications, such as tachyarrhythmic cardiomyopathy, myocardial infarction, heart failure with preserved ejection fraction (HFpEF), and sudden cardiac death. Catheter ablation (CA) is indicated in patients with drug-refractory or symptomatic AF, with pulmonary vein isolation (PVI) being the treatment of choice. Successful PVI requires transseptal puncture (TSP) to allow left atrial (LA) access. A potential obstacle during TSP is patent foramen ovale (PFO) occluder. PFO occluder implantation is performed in selected patients with PFO for secondary prevention of cryptogenic stroke [1].
We present an image of successful PVI in a patient with a PFO occluder, in whom TSP was performed using 14 French (Fr) sheath under transesophageal echocardiography (TEE) guidance.
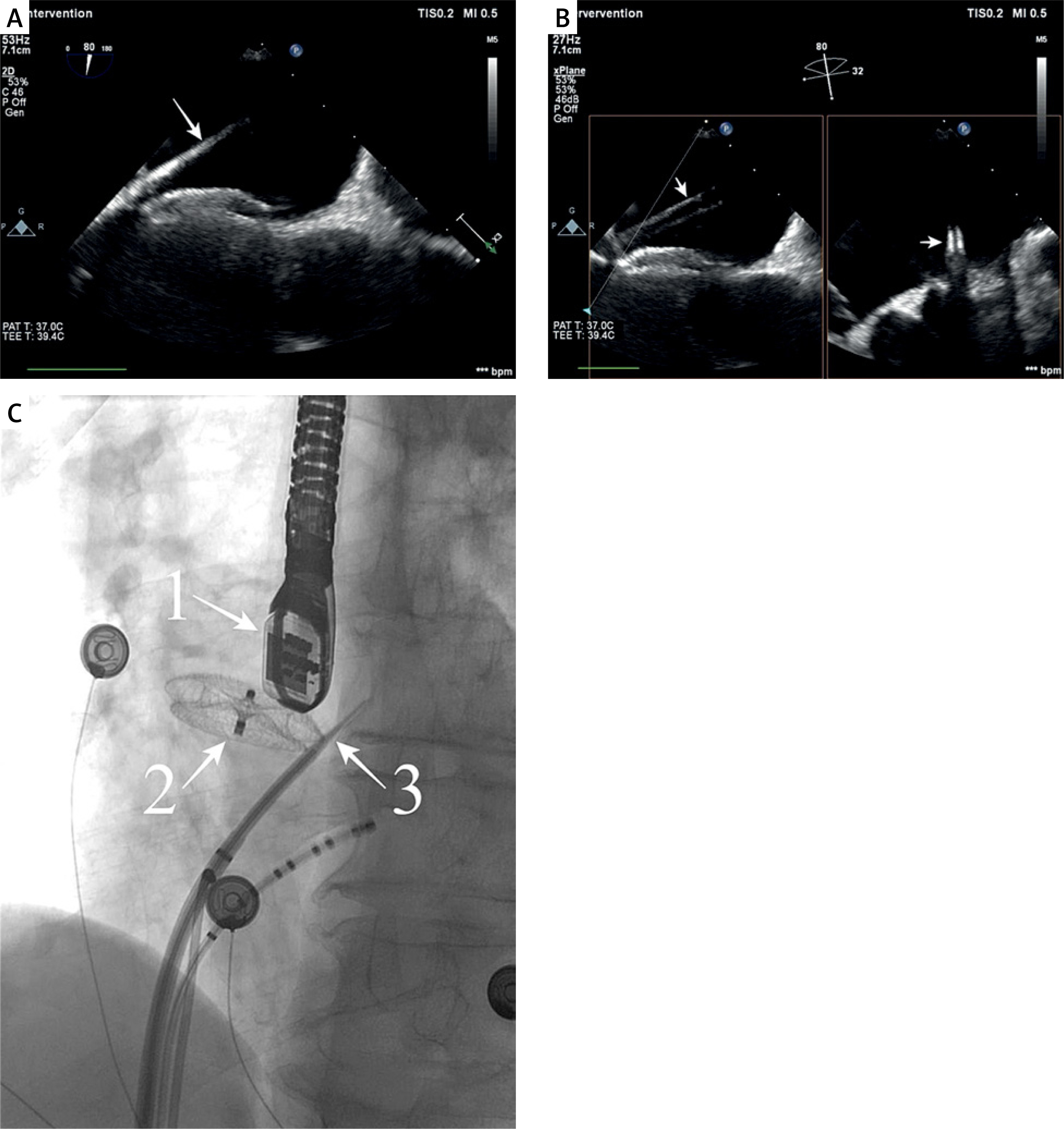
A 60-year-old patient with a history of persistent AF was admitted to the electrocardiology department for CA. He had experienced three AF episodes, each requiring an electrical cardioversion. Comorbidities included HF, hypertension, hypercholesterolemia, asthma, and a history of ischemic stroke in 1997, and Amplatzer 19-mm PFO occluder implantation in 2021 for stroke secondary prevention. Pre-procedural transthoracic echocardiography (TTE) demonstrated a small LA (area 14 cm2, diameter 37 mm). Intraprocedural TEE excluded LA thrombi. Afterwards, a non-steerable sheath (8 Fr) and TSP needle were advanced to the superior vena cava. Under atrial pressure monitoring, combined TEE and fluoroscopy guidance, TSP was performed (Figure 1). The TSP was confirmed with a contrast administration. A sheath exchange for Faradrive sheath (14 Fr) was performed over-the-wire to maintain sheath position and enhance procedural safety. The PVI was performed using a Farawave catheter. Post-procedural TTE showed no pericardial effusion. The procedure lasted 45 min, fluoroscopy 10:41 min, and the radiation dose was 283 mGy, including rotational angiography of LA and PVs. The patient was discharged the following day.
Figure 1
A – Intraprocedural transesophageal echocardiography – the needle passing through the interatrial septum, below the occluder (arrow). B – Intraprocedural TEE – transseptal sheath passing through the interatrial septum (arrows). C – Intraprocedural fluoroscopy view of transseptal puncture (1 – echocardiography probe, 2 – occluder, 3 – transseptal needle)
The evidence on the feasibility and safety of TEE-guided TSP in patients with septal occluders remains limited. A multicenter prospective observational study evaluating the safety of TSP reported that most punctures were performed with a steerable sheath via the posterior-inferior segment of the interatrial septum. Preprocedural imaging, including computed tomography (CT), magnetic resonance imaging, or fluoroscopy, was performed to facilitate planning [2]. In another single-center study assessing the safety of TSP in patients with occluders, the fluoroscopy was the primary imaging modality. TEE was reserved for patients with PFO occluder poorly visualized by fluoroscopy [3]. In another report, CT was used prior to CA to visualize the occluder position, while TSP was performed under TEE [4].
Our report shows that intraprocedural TEE ensures feasible TSP in patients with septal occluders without performing additional preprocedural imaging, limiting the fluoroscopy dose. TEE guidance is valuable when large sheaths are used, as precise imaging is essential in these cases.
TEE provides high-resolution imaging of interatrial septum and LA allowing precise localization of septal occluders and safe navigation during TSP. Our case demonstrates that TEE-guided TSP with a large-bore 14 Fr sheath is a feasible approach in patients with PFO occluders undergoing PVI.